The Science of TMJ Pain: Understanding Ear Pain and Jaw Connection
Explore the link between TMJ and ear pain, offering insights into effective management.
You know the feeling: your jaw pops, your ear aches, and Google lists a dozen scary causes before breakfast. The culprit might be the temporomandibular joint (TMJ), that tiny hinge letting you chew pizza. Recent research is exploring why jaw trouble often masquerades as ear trouble. If you grind your teeth, wake up with headaches, or suspect an ear infection that never appears on a lab test, this article is for you.
Buckle up for an evidence-based tour of the TMJ, its surprising ear connection, and practical strategies to keep both areas quiet. We will keep the jargon light and the science solid, leaning on peer-reviewed studies and reputable medical sources to help you separate myths from facts.
The Anatomy of the Jaw: Understanding TMJ
TMJ Structure and Function
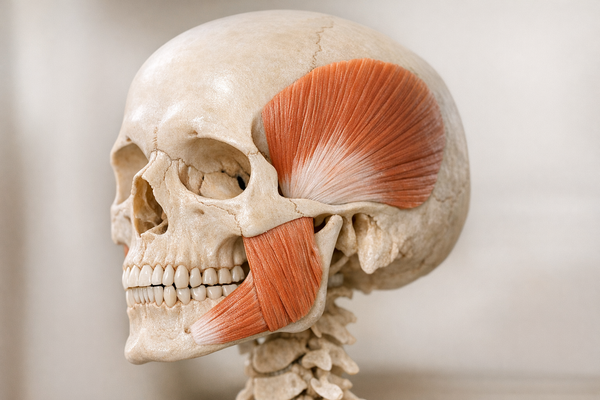
Your TMJ sits right in front of each ear where the lower jaw (mandible) meets the temporal bone of your skull. Think of it as a sliding-hinge combo. The joint consists of a bony socket, the mandibular condyle, and a thin cartilage disk that cushions motion. A web of ligaments, muscles, and nerves keeps everything coordinated so you can talk, chew, and yawn without thinking.
Developmentally, the TMJ is a late bloomer. A 2024 study by Fernández-Rubio and Radlanski found that the secondary jaw joint continues to mature into adolescence, making it sensitive to habits like clenching and grinding. When that disk gets displaced or the cartilage wears down, pain often travels along the nearby trigeminal and auriculotemporal nerves—key pathways between your jaw joint and brain.
The joint can also deteriorate from external stress. A review of TMJ prosthetic failures by Ghaly and colleagues highlights how chronic stress can lead to bone erosion, disk perforation, and sometimes artificial joint replacement if conservative care fails. Learn more about how stress exacerbates bruxism and jaw tension.
While teeth and cartilage get most of the attention, remember the supporting cast. The lateral pterygoid muscle, for instance, pulls the jaw forward with every bite and is one of the first to spasm under stress. Physical therapists often call it the “silent troublemaker” because it sits so deep you rarely feel it directly—yet it can tilt the disk out of its normal track in one night of hard grinding.
Why TMJ Matters
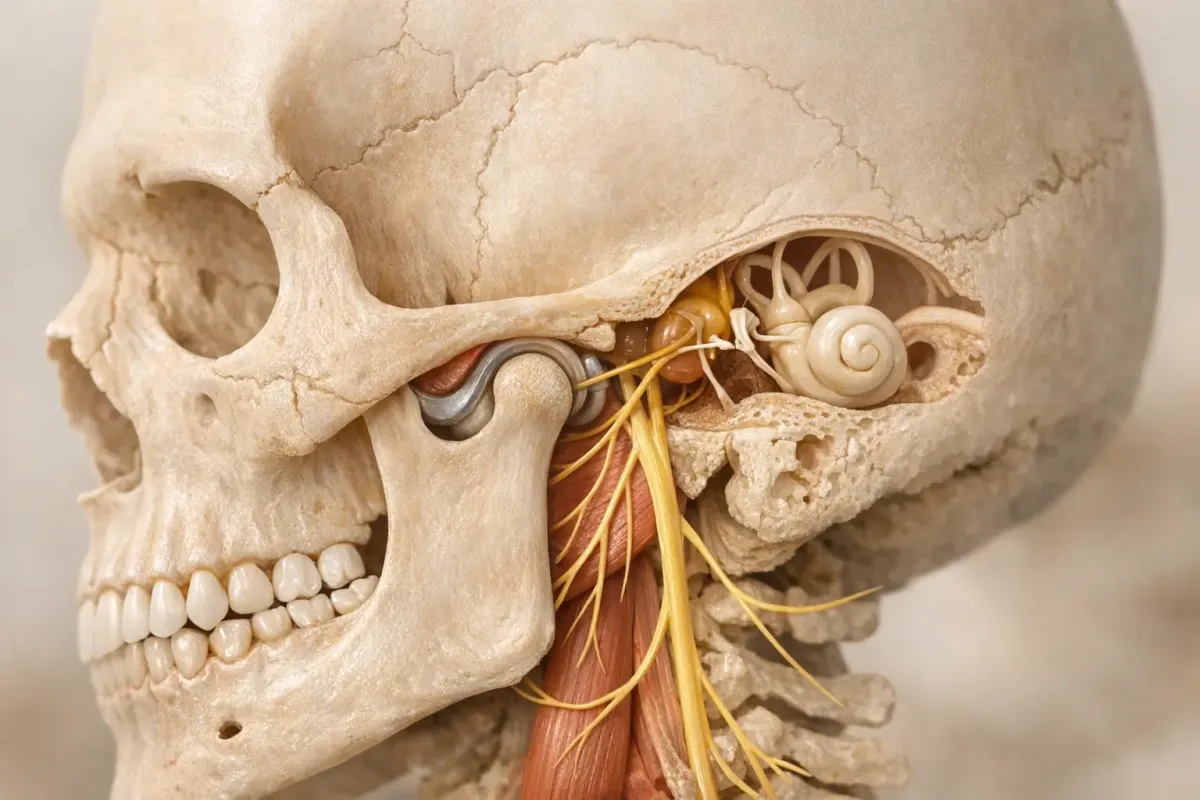
The TMJ endures more stress than you might think. It can sustain forces greater than 200 pounds when you clench—about the weight of a barbell plate. Add nightly tooth grinding (bruxism), bite misalignment, or injury, and the load climbs higher. Because the joint is millimeters from the ear canal, any swelling or nerve irritation in the TMJ can radiate pain into the ear, temple, and neck.
If you spend the day hunched over a laptop, chew gum like it’s cardio, or sleep with your jaw locked, you are asking a small joint to do big-time heavy lifting. Understanding how the TMJ works is the first step in figuring out why your “earache” might be jaw-driven instead of infection-driven.

Ear Pain and TMJ Disorders: What's the Connection?
Mechanisms Linking Ear and Jaw Pain
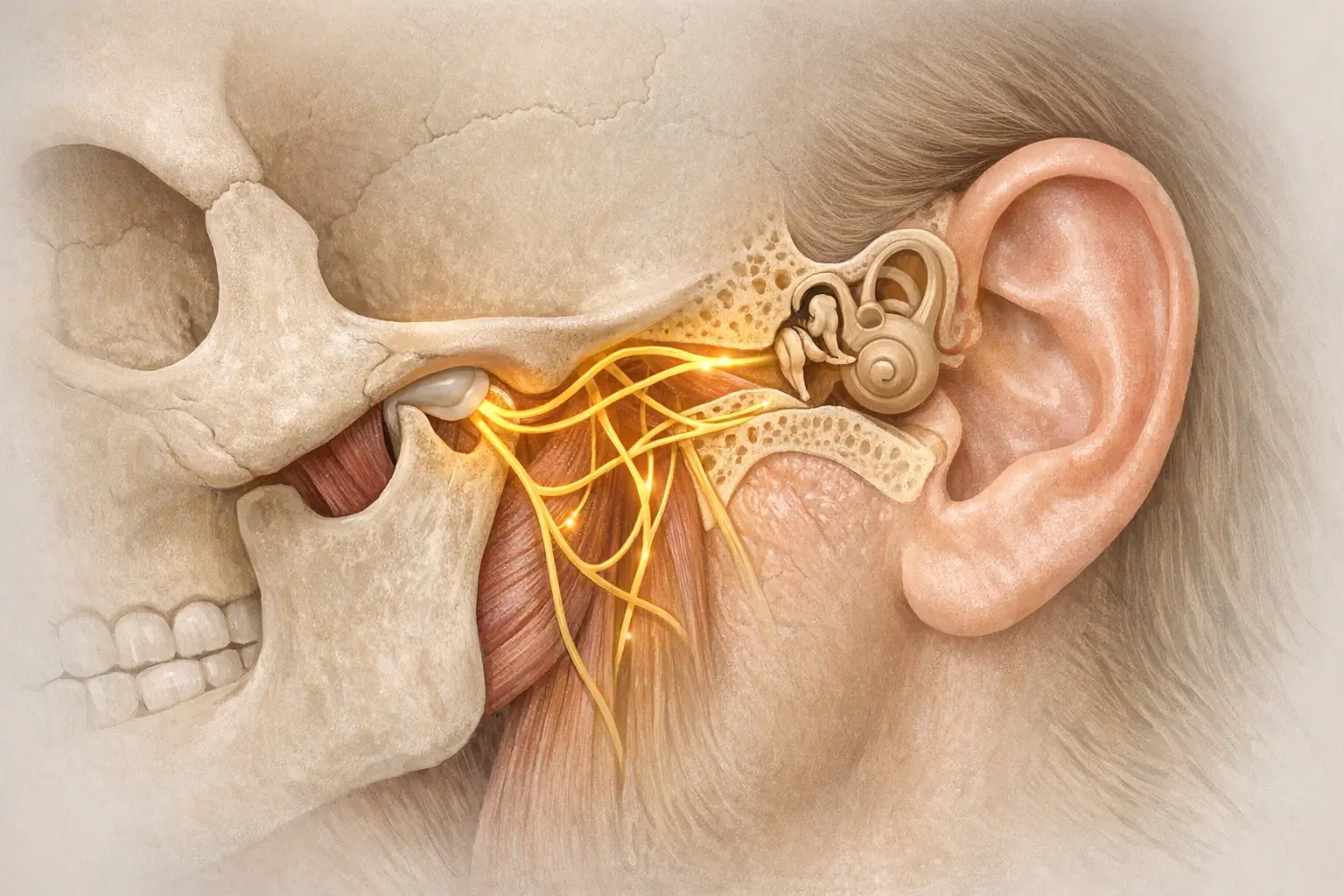
The ear and jaw share not only space but also nerve supply. The auriculotemporal nerve branches from the mandibular division of the trigeminal nerve and feeds sensation to both the TMJ and parts of the external ear canal. When inflammation hits the joint capsule, pain signals can short-circuit to the ear.
A 2025 systematic review by Osiewicz and Więckiewicz mapped how biochemical irritants like cytokines leak from an inflamed TMJ into adjacent tissues, activating pain receptors in the ear. The authors also note that jaw clenching spikes intra-articular pressure, similar to squeezing a balloon next to your ear’s pain fibers. Explore more about ear pain linked to TMJ and bruxism.
On the mechanical side, the TMJ’s disk and ligaments tug on the same fascia that anchors tiny middle-ear muscles. When the disk slips forward, it can yank those muscles, creating a dull earache without any infection. A 2024 analysis in the Journal of Oral Rehabilitation found that patients with disk displacement reported ear pain 62% of the time, versus 12% in controls with healthy disks.
Case Studies and Real-Life Implications
Consider Sarah, a 35-year-old marketing manager who frequently visited her ENT clinic with “recurring ear infections.” Cultures were clean, but her pain flared during budget season. The turning point came when her dentist noticed flat molar surfaces—a tell-tale sign of bruxism. After a night guard and jaw exercises, her “ear infections” vanished.
Another case from Johns Hopkins Medicine profiles a violinist whose intense chin-rest pressure jammed her jaw backward, causing tinnitus and ear fullness. When a physical therapist realigned her posture and taught relaxation drills, the ear symptoms eased within weeks.
Stories like these align with data. A cross-sectional study of 312 patients published by the Cleveland Clinic reported that 42% of people seeking care for “chronic ear pain” ended up with a primary TMJ diagnosis rather than an ear-related one.
Symptoms and Diagnosis: Identifying TMJ-Related Ear Pain
Common Symptoms
TMJ trouble rarely shows up alone. You might notice:
- Ear pain or fullness without infection
- Clicking, popping, or grinding noises when opening or closing your mouth
- Headaches around the temples
- Jaw stiffness, especially in the morning
- Difficulty chewing chewy foods or wide yawning
- Occasional dizziness or ringing in the ears (tinnitus)
- Soreness when pressing gently in front of the ear canal
Dental researchers van Gessel and de Rijk documented in their 2024 report that nearly half of post-dental-treatment TMJ cases first presented as unexplained ear discomfort. Meanwhile, orthodontic data by Solomon et al. link malocclusion with early cartilage wear, amplifying joint clicks and ear pain. For more on jaw pain on one side, check our detailed guide.
Diagnostic Techniques
Getting the right diagnosis can save you from unnecessary antibiotics. Here is how clinicians usually proceed:
- History check. They will ask about jaw clenching, trauma, gum chewing, stress, and dental work.
- Physical exam. Gentle palpation of the joint while you open and close your mouth can reveal tenderness or crepitus (crackling sounds).
- Auscultation. Some dentists use a stethoscope to detect hidden clicks.
- Imaging. Panoramic X-rays rule out fractures, while MRI shows soft-tissue details like disk displacement. CBCT (cone beam CT) gives a 3-D view of bone changes.
- Rule-out tests. Tympanometry or an otoscopic exam by an ENT can confirm your eardrum is intact, steering the focus back to the jaw.
You can also perform a quick at-home screen: place two fingers on the joint in front of your ears, open wide, then close. If one side clicks or feels tender, flag it to your dentist. Self-checks never replace a clinical exam, but they help you track patterns between jaw motion and ear symptoms.
Advanced centers sometimes add surface electromyography (sEMG) to measure muscle hyperactivity. Johns Hopkins lists this as optional but helpful for night-time bruxers who swear they “sleep fine.”
Effective Management Strategies for TMJ and Ear Pain
Nonsurgical Treatments
Most TMJ-related ear pain calms down with conservative care. A 2024 review by Madhuri, Suresh, and Tikoo found that 75% of patients achieved “clinically meaningful pain relief” within three months of nonsurgical therapy. Options include:
- Occlusal splints (night guards). Custom acrylic devices reduce tooth wear and distribute jaw forces evenly.
- Physical therapy. Targeted stretches (like the “goldfish exercise” and controlled chin tucks), posture drills, and manual mobilization free up joints and relax overworked muscles. Discover more on physical therapy's role in TMJ relief.
- Medication. Short courses of NSAIDs, muscle relaxers, or low-dose tricyclics can reduce inflammation and nerve hypersensitivity.
- Dry needling or trigger-point injections. These calm muscle knots in the masseter and temporalis that refer pain to the ear. Explore dry needling as a novel TMJ relief method.
- Cognitive-behavioral therapy. Stress management reduces clenching episodes. Remember, your jaw is often your stress ball. Learn more about CBT and mindfulness for bruxism.
According to the National Institute of Dental and Craniofacial Research, splints worn at night have a 60 to 90% success rate, especially when combined with daytime habit coaching.
Real-world tip: Schedule micro-breaks on your phone every 45 minutes. When the alarm buzzes, rest your tongue lightly behind your front teeth, drop your shoulders, and let the lower jaw hang for ten seconds. Users in a 2023 physiotherapy audit cut self-reported clench time by nearly one-third with this trick alone.
Surgical Interventions
Surgery is the last resort, not the first. The same Madhuri review cautions that open-joint procedures carry higher complication rates than arthroscopy. Candidates usually have severe disk degeneration, bone spurs, or ankylosis (joint fusion). Techniques range from:
- Arthrocentesis. Saline flushing and hydraulic lysis of adhesions.
- Arthroscopic disk repositioning. Minimally invasive suture or anchor repairs.
- Open-joint replacement. Total alloplastic prosthesis for end-stage destruction. Note: failure rates and revision challenges were cataloged by Ghaly et al..
The rehab clock does not stop in the operating room. Surgeons typically prescribe six weeks of graduated mouth-opening exercises using stackable tongue depressors or silicone wedges. Skipping this phase can lead to scar tissue and recurring problems.
The Role of Lifestyle Changes
Your daily routine can either sabotage or support recovery. An interdisciplinary program at Dr. M. Djamil General Hospital in Indonesia reported by Gunawan and Sahputra reduced pain scores by 43% after 12 weeks of combined dental, physiotherapy, and psychological care. Key lifestyle tweaks include:
- Switching to softer foods for a few weeks, then gradually introducing firmer textures.
- Limiting gum, jerky, and wide bites (watch out for triple-stack burgers).
- Practicing jaw-relaxation drills every hour: lips together, teeth apart, tongue on the roof of the mouth. Discover more on natural jaw tension relief.
- Using heat packs for 15 minutes before bed to relax tight muscles.
- Tracking stress triggers in a journal and pairing each with a non-jaw outlet like deep breathing or a quick walk.
If you’re a side sleeper who struggles to change, try hugging a pillow in front of your chest; it prevents you from burying your chin into the mattress, which jams the jaw backward toward the ear canal.
Prevention and Long-Term Management
Daily Habits to Reduce TMJ Strain
Preventing flare-ups is more cost-effective than treating them. Start with these habits:
- Desk posture. Keep your monitor at eye level and shoulders relaxed. Forward-head posture increases muscle tension around the jaw and ear. Understand more about posture's impact on jaw pain.
- Micro-breaks. Every 30 minutes, unclench and move your jaw gently side to side.
- Sleep savvy. Back sleeping with a small support pillow under the neck reduces side pressure on the jaw.
- Bite awareness. Catch yourself when you clamp your teeth while texting or driving.
- Regular dental checks. Early adjustment of high fillings or crooked crowns prevents uneven bite forces.
- Hydration and nutrition. Well-lubricated cartilage needs water and collagen-building nutrients such as vitamin C. Dehydrated disks wear faster.
The orthodontic osteoarthritis study by Solomon et al. emphasizes that early alignment fixes reduce the risk of long-term cartilage wear, decreasing both jaw and ear complaints.
Monitoring and Follow-Up
Even after symptoms fade, keep tabs on your TMJ like you would on blood pressure. Periodic check-ups allow your provider to tweak splints, monitor muscle tension, and refresh exercise programs. The interdisciplinary protocol outlined by Gunawan and Sahputra schedules reviews at 3, 6, and 12 months, catching small relapses before they balloon.
Some apps now let you log clench episodes, just like counting steps. If you notice a stress-jaw pain pattern, loop in your therapist or coach early. Prevention is a team sport.
Conclusion
Your jaw and ear are partners in crime, sharing nerves, muscles, and the occasional pain signal. Research—from developmental anatomy [6] to treatment outcomes [9]—shows that TMJ disorders commonly present as ear pain. The good news: most cases respond well to conservative care, smart lifestyle tweaks, and an interdisciplinary mindset.
If you feel an unexplained earache brewing, pause before you reload that antibiotic prescription. Check in with your jaw: Is it clenched? Does it click? Have you been stress-chewing through deadlines? A quick self-audit could spare you months of confusion—and provide a clear action plan with proven success rates.
Next time your ear throbs but your ENT visit turns up empty, consider giving your jaw the spotlight. Understanding the science helps you pick targeted, evidence-backed strategies so you can chew, speak, and sleep without that nagging ache. Your ears—and your pizza nights—will thank you.