Understanding TMJ: How Sleep Disorders Contribute to Jaw Pain
Explore the link between TMJ and sleep disorders, focusing on jaw pain management.
You wake up with a dull ache near your ear, a pop in your jaw, or a headache that seems to start right behind your molars. Somewhere between counting sheep and hitting the snooze button, your temporomandibular joint (TMJ) decided to throw a tantrum. If you also snore, grind, or stop breathing for short bursts during the night, the plot thickens. Mounting research suggests that sleep disorders and jaw pain are frenemies that love to ruin a good night’s rest and your mornings too. Studies by Greenbaum et al. and Maniaci et al. highlight these connections.
This article walks you through the science of that annoying click in your jaw, the nighttime grinding that fuels it, and the treatments that might finally let you greet the day without clenching your teeth. No fluff, just evidence, a bit of cheek, and a roadmap you can actually use.
The Basics of TMJ and Sleep Disorders
Defining TMJ
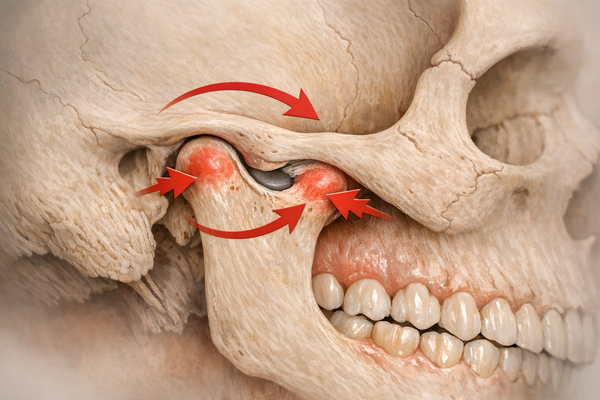
Your TMJ is the sliding hinge that connects your lower jaw to the skull. The joint is a small marvel. A fibrous capsule houses a cartilage disk that cushions movements in three dimensions—opening, closing, and slight side-to-side glides when you chew that stubborn piece of sourdough. When this disk or the muscles around it misbehave, you get temporomandibular disorders (TMD). Symptoms range from clicking sounds to difficulty chewing, pain spreading to the neck, and those pesky tension headaches. According to the National Institute of Dental and Craniofacial Research, around 10 million Americans report TMJ issues each year, with women accounting for most cases.
Because the jaw is wired with nerves close to the ear canal, a single irritated muscle can feel like a concert of discomfort. Earaches, facial pain, and even dizziness roll into one. A study by Greenbaum et al. explored how jaw muscle function overlaps with sleep breathing problems, suggesting that your airway and your bite may share the same bad habits.
Common Sleep Disorders
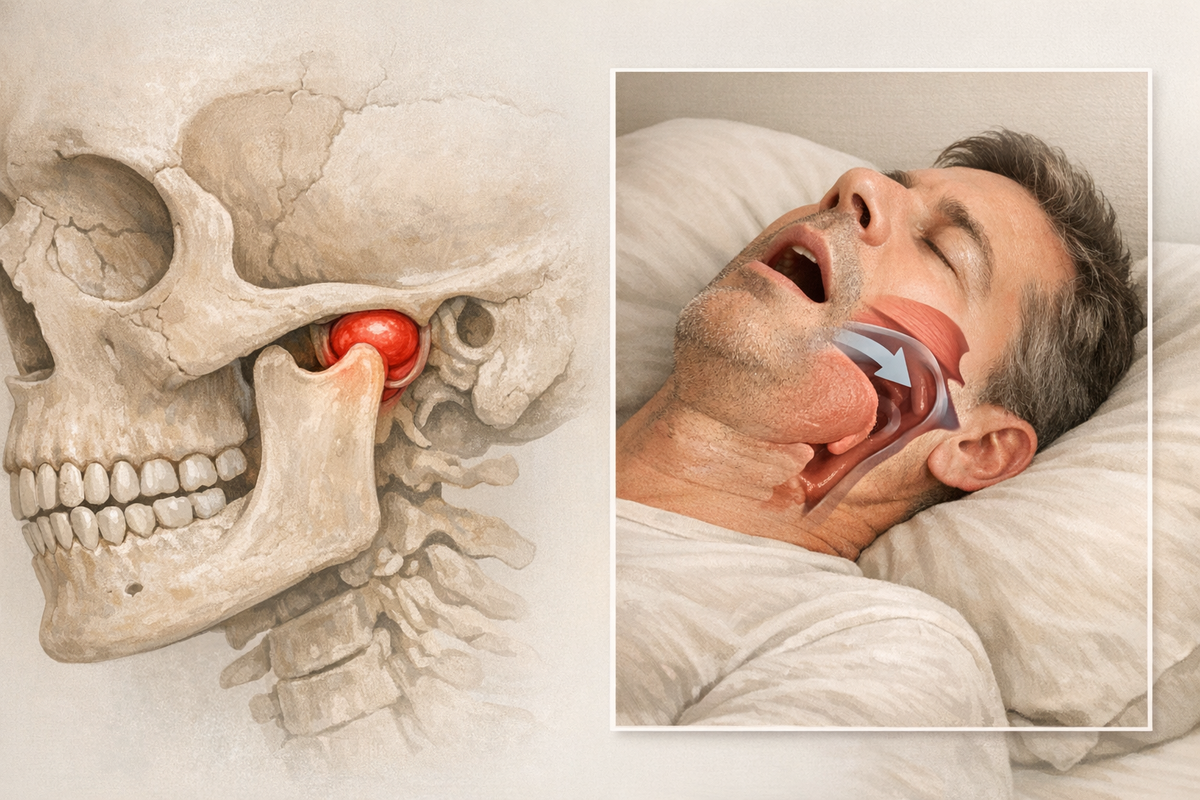
Sleep disorders come in many flavors, but obstructive sleep apnea (OSA) and bruxism get the most side-eye from dentists and sleep docs. OSA occurs when throat muscles relax too much, cutting off airflow. You gasp, snore, or briefly wake up and repeat all night. An extensive review in Sleep Medicine by Maniaci et al. pegs OSA prevalence at roughly 10 percent in adults.
Bruxism, the star of involuntary tooth grinding or clenching, shows up in about 8–13 percent of adults and as high as 20 percent in children, based on updates summarized in the consensus report by Verhoeff et al. Add stress, caffeine, or misaligned teeth, and your odds climb even higher. To explore how stress can exacerbate bruxism, you might find this article on how stress worsens bruxism insightful.
Both OSA and bruxism rob you of deep sleep. They also put your jaw muscles through a workout no fitness coach would endorse, setting the stage for pain. In practical terms, that means nodding off at your desk, afternoon brain fog, and a jaw that feels like it chewed through a bag of rocks.

The Jaw Pain Sleep Connection
How Sleep Disorders Affect Jaw Pain
When your airway narrows during OSA, your brain sends a panic signal: “Open wider.” The lower jaw reflexively shifts forward to open the airway. That repetitive jaw thrust can overwork the muscles that hinge your TMJ. Meanwhile, bruxism pumps up muscle tension through thousands of tiny contractions per night. In one hour of grinding, your masseter muscles can exert forces up to 250 pounds per square inch. No wonder they protest in the morning. For more on how sleep positions can exacerbate jaw pain, check out this guide on sleep positions and bruxism.
A clinical overview by Patil et al. reported that roughly half of patients with chronic orofacial pain also showed sleep apnea markers. They found jaw pain intensity rose with the severity of apnea events. Another randomized trial tested whether treating sleep apnea could change TMJ symptoms. Attia et al. noted in their trial that jaw pain improved in patients who used mandibular advancement devices compared with those on CPAP alone.
Mechanisms Involved
- Muscle Hyperactivity: Micro-arousals in OSA and bruxism trigger bursts of jaw muscle activity. Over time, this causes fatigue, micro-tears, and inflammation.
- Nerve Sensitization: Repeated strain on the TMJ can sensitize the trigeminal nerve. That makes everyday chewing or even talking feel painful.
- Reduced Oxygen: OSA’s intermittent oxygen dips may starve local tissues, hindering muscle repair and amplifying pain perception.
- Postural Chain Reaction: Jaw protrusion to open the airway often tilts the head and tenses neck muscles, creating a full-body posture puzzle that feeds back into the TMJ.
- Inflammatory Cascade: Cytokines such as IL-6 and TNF-α flood the joint space after repeated mechanical stress, turning short-term aches into chronic pain.
Understanding these overlapping pathways helps clinicians tailor treatments that tackle both sleep quality and jaw mechanics rather than addressing them in isolation.
Bruxism: The Nighttime Grind
What is Bruxism?
Bruxism is more than grinding teeth like a villain in a cartoon. The updated definition from the International Consensus Meeting describes it as a “masticatory muscle activity during sleep or wakefulness” characterized by clenching, bracing, or thrusting. Sleep bruxism is classified as a movement disorder linked to arousal responses, whereas wake bruxism is often stress driven.
Kids grind too. A narrative review by Leung et al. highlights prevalence rates in children between 14 and 20 percent, especially during growth spurts. Pediatric dentists now routinely screen for tell-tale flattened molar cusps during six-month check-ups. For parents, understanding pediatric bruxism can be critical in managing early symptoms.
Impact on Jaw Health
Grinding vibes send shockwaves from your teeth to the TMJ. Here is what chronic bruxism does:
- Enamel Wear: Without the tooth’s natural cushion, force travels straight to the joint.
- Disk Displacement: The cartilage disk inside the TMJ can slip out, causing clicking or locking.
- Muscle Hypertrophy: Over time, masseter muscles bulk up like overtrained biceps, which can stiffen the joint and limit motion.
- Inflammation: Micro-trauma sparks inflammatory chemicals that make the joint sensitive.
Adults with bruxism frequently develop morning headaches, ear aches, and limited jaw opening. Dental occlusion patterns in bruxers differ too. A cross-sectional analysis by Cadar and Almăşan pinpointed high-angle bites that shift load onto the TMJ. For those dealing with bruxism, exploring natural bruxism solutions can offer alternative management strategies.

Research and Clinical Insights
Key Studies on TMJ and Sleep Disorders
Let us break down the major findings without burying you in jargon.
- Jaw Function Meets Airway Study
The study by Greenbaum et al. used electromyography to measure jaw muscle fatigue in OSA patients. Results showed that those with severe apnea had 30 percent lower muscle endurance compared to controls. Translation: your airway fight tires out your jaw before breakfast. - Orofacial Pain and Sleep Apnea Review
Patil et al. pooled data from 18 trials totaling 1,245 patients. They found that treating OSA reduced orofacial pain scores by an average of two points on a ten-point scale. Pain relief kicked in within six weeks of consistent therapy. - Splint vs Botulinum Toxin Trial
In 2024, Chisini et al. randomized 80 probable sleep bruxism sufferers to either a nighttime occlusal splint or targeted botulinum toxin-A injections. After three months, both groups enjoyed reduced pain, but the splint group saw a 40 percent drop in grinding episodes, suggesting mechanical devices may blunt the cause as well as the symptom.
The convergence is clear: healthier sleep equals happier jaws, and vice versa. This dual focus is pushing clinics to set up interdisciplinary “sleep-orofacial” teams where dentists, ENT surgeons, and physical therapists hash out treatment plans together.
Managing Jaw Pain Linked to Sleep Disorders
Treatment Options
No one-size-fits-all magic bullet exists, but you have choices.
- Mandibular Advancement Devices (MADs)
For mild to moderate OSA, custom MADs hold your jaw forward a few millimeters, opening the airway and reducing apnea events. The trial by Attia et al. showed MADs trimmed nighttime jaw pain episodes by 35 percent versus CPAP alone. - Occlusal Splints
Think of these as helmets for your teeth. They spread bite force evenly and let muscles relax. In the study by Chisini et al., splints outperformed placebo at lowering pain scores in probable bruxism. Understanding how mouth guards compare to other treatments can help in choosing the right solution. - Botulinum Toxin-A
Micro-doses injected into the masseter or temporalis muscles can reduce clenching strength. The same randomized trial found pain relief comparable to splints, though grinding episodes did not drop as much. - Physical Therapy
Manual release techniques, ultrasound, and guided mobility drills can ease trigger points around the TMJ and neck. A small pilot by Martínez et al. reported a 50 percent drop in pain scores after six weekly sessions. The role of physical therapy in TMJ and bruxism relief is increasingly recognized. - Continuous Positive Airway Pressure (CPAP)
CPAP still rules for moderate to severe OSA. By stabilizing oxygen levels, it can decrease nighttime arousals that fuel jaw movements.
Lifestyle Modifications
You can tweak daily habits to give professional treatments a boost.
- Sleep Hygiene: Stick to a set bedtime, darken the room, and cool it down to 65 °F. Fewer arousals equal fewer grinding bursts. Learn more about how sleep hygiene can reduce bruxism.
- Stress Management: Mindfulness apps, yoga, or even a brisk walk after work can drop clenching intensity. The American Dental Association notes a clear link between stress and wake bruxism.
- Limit Alcohol and Caffeine: Both loosen airway muscles and spike muscle activity. Cut them off at least four hours before bed. For more on this, read about why you should avoid caffeine late at night.
- Jaw Exercises: Try “controlled opening” (slowly open to halfway, hold for five seconds, close) and “tongue-up” posture (resting tongue on palate) ten times each night. Consistency teaches muscles to idle rather than fire.
- Posture Checks: An ergonomic workstation keeps head and neck aligned, taking extra load off the TMJ. A sticky note on your monitor reading “uncurl your chin” works wonders.
Combine two or three of these strategies and you often see pain scores tumble within a month. Keep a symptom diary—many patients are surprised to learn that the week they ditched late-night espresso was the week their clicking lessened.
Future Directions in Treatment and Research
Emerging Therapies
Scientists are tinkering with new ways to calm hyperactive jaw muscles and stabilize the airway.
- Pharmacologic Targets: A review on FTO proteins by Li et al. suggests epigenetic pathways could modulate inflammatory responses in oral tissues. While still in petri dishes, small-molecule inhibitors may one day dial down TMJ inflammation.
- Digital Bruxism Monitors: Wearables that measure bite force in real time are in pilot testing. They could cue relaxation audio whenever you clench, creating biofeedback loops. Think Fitbit, but for your jaw.
- Neuromodulation: Low-level transcutaneous electrical nerve stimulation (TENS) during sleep is under study for reducing nocturnal muscle bursts.
- 3-D Printed Oral Appliances: Rapid prototyping can produce lighter, thinner MADs custom-shaped to a patient’s scan in under 24 hours, slashing adjustment visits.
Research Gaps
Despite the progress, several questions remain.
- Standardized Diagnostics: The Standardised Tool for Bruxism Assessment by Manfredini et al. aims to unify criteria but is not yet globally adopted. Until everyone measures the same way, comparing studies is like matching apples to oranges.
- Pediatric Long-Term Data: We know kids grind, but do childhood patterns predict adult TMJ disorders? Longitudinal studies are sparse.
- Combination Therapies: Few trials test CPAP, splints, and physical therapy together. Real-world care is multidisciplinary, so research should mirror it.
Conclusion
Your TMJ and your sleep habits are locked in a nightly tug-of-war. Obstructive sleep apnea pushes your jaw forward to breathe, while bruxism clamps it shut in rhythmic bursts. Over time, these forces inflame joints, tire muscles, and leave you wincing over morning coffee.
The good news is that evidence-based tools—from mandibular advancement devices to stress management and smarter sleep hygiene—can break the cycle. Studies like those by Greenbaum, Patil, and Chisini draw a clear map: treat the sleep disorder, protect the jaw, and the pain usually backs off.
If you suspect your jaw pain is more than “just stress,” talk with both a dentist and a sleep specialist. A coordinated plan that tackles airway, muscle load, and lifestyle delivers the best odds of waking up pain-free—without grinding through another night.