Exploring Muscle Relaxants for TMJ Pain Relief: An Evidence-Based Approach
Discover how muscle relaxants can provide TMJ pain relief with evidence-based insights.
If your jaw pops louder than vintage bubble wrap or aches after a night of tooth-grinding, you might have searched for “TMJ pain” at 2 a.m. The search results can be confusing—TMD, NSAIDs, CBT, BoNT. This article clarifies the role of muscle relaxants in temporomandibular joint (TMJ) pain using evidence-based insights. You will learn what the science says, what these medications do, and when combining them with exercise or lifestyle changes might be beneficial. For those interested in alternative approaches, our article on innovative TMJ treatments might be useful.
Every claim is backed by peer-reviewed studies or authoritative institutions like the Mayo Clinic. No hype, no myths—just the data you need before consulting your dentist, doctor, or that friend who swears by coconut oil.
Understanding TMJ Disorders and Pain
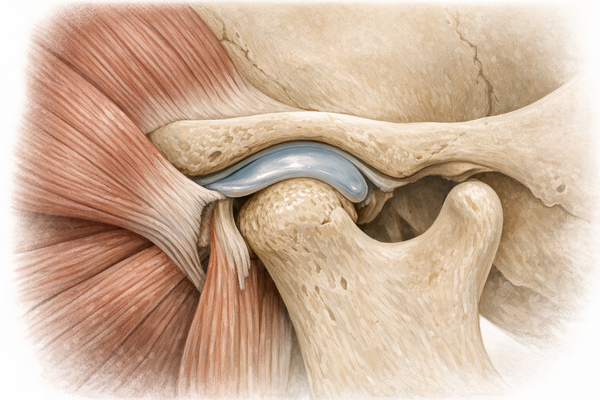
The temporomandibular joint is the sliding hinge that connects your jawbone to your skull. Problems with this joint lead to temporomandibular disorders (TMD). According to the National Institute of Dental and Craniofacial Research, up to 10 percent of adults experience TMD symptoms. An evidence map from a 2025 narrative review by Jogna et al. highlights pain, joint noises, and limited mouth opening as common complaints.
Jaw issues are not just a mouth problem. They can cause headaches, ear pain, or neck stiffness, making chewing, yawning, and even talking feel like a workout for your face. Untreated TMD can disturb sleep, increase stress, and reduce focus—especially for those with sleep bruxism who grind their teeth at night. Learn more about the connection between sleep disorders and bruxism to understand the broader impact on jaw pain.
Causes of TMJ Pain
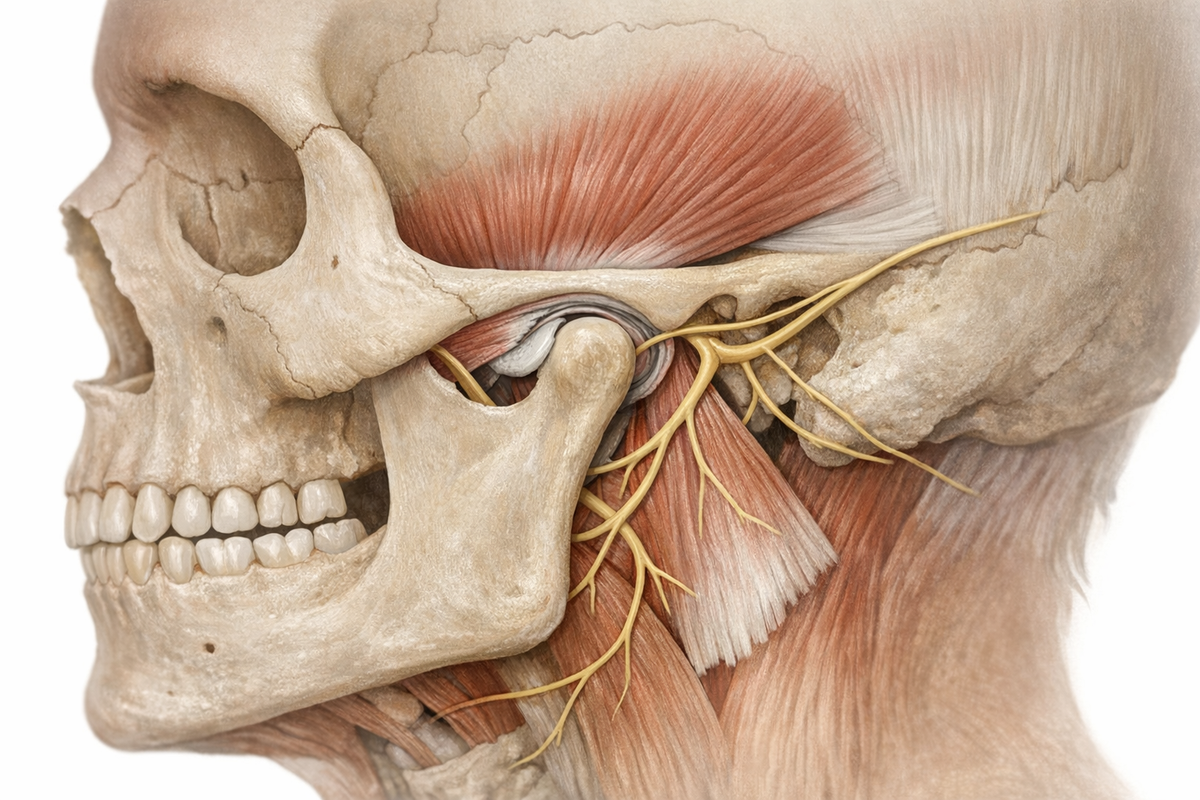
- Bruxism: Clenching or grinding at night strains the masseter and temporalis muscles. A network meta-analysis by Christidis et al., 2024, lists bruxism as a primary driver of myofascial pain within TMD. For strategies to prevent grinding, visit our guide on how to stop grinding teeth in sleep.
- Trauma: Injuries like a punch, fall, or whiplash can damage the joint disk or ligaments.
- Arthritis: Osteoarthritis or rheumatoid arthritis can erode joint structures.
- Posture and Stress: Poor posture and stress-induced grinding increase muscle tension around the jaw and neck. Explore how jaw tension from stress can further exacerbate TMJ pain.
- Dental Factors: Issues like malocclusion can shift load to the TMJ, as reviewed by Yadfout et al., 2024.
Symptoms to Watch For
Recognizing symptoms early is crucial. Look out for:
- Jaw pain or tenderness, especially in the morning
- Clicking, popping, or grinding sounds when opening the mouth
- Limited range of motion or jaw locking
- Facial pain that radiates to the temple or ear
- Headaches and neck tightness
- Sore teeth without obvious cavities (a sign of bruxism)
When these symptoms appear, your care team may consider pharmacological options like muscle relaxants, alongside mouth guards. This is where it gets interesting. For more on this, check out our TMJ mouth guard guide for choosing the right guard.

Muscle Relaxants in TMJ Pain Management
Muscle relaxants calm hyperactive jaw muscles, reduce spasms, and interrupt pain feedback loops. Patel and Ouanounou's 2026 review analyzed 17 clinical trials, finding that about 60 percent of patients taking cyclobenzaprine or tizanidine reported a 30 percent pain reduction after four weeks. This relief is similar to non-steroidal anti-inflammatory drugs (NSAIDs) but with a different mechanism.
A 2024 network meta-analysis by Christidis et al. ranks muscle relaxants among the top pharmacological options for reducing myofascial TMD pain, ahead of benzodiazepines and topical lidocaine. So, evidence supports their use when chosen wisely.
How Muscle Relaxants Work
Most oral muscle relaxants act centrally. They don't target the jaw directly but dampen nerve firing in the brainstem and spinal cord, reducing muscle contractions. It's like turning down the volume on a loud guitar amp before the neighbors complain. If you're considering non-drug options, read about natural bruxism solutions that can complement your treatment plan.
- Cyclobenzaprine: A tricyclic compound that blocks alpha-motor neurons, reducing hyperactivity.
- Tizanidine: An alpha-2 adrenergic agonist that reduces muscle tone and also has mild analgesic effects.
- Baclofen: A GABA-B receptor agonist that limits spasticity, though it can cause sedation.
Each drug has its quirks—cyclobenzaprine can cause grogginess, tizanidine may lower blood pressure, and baclofen can induce dizziness. You and your doctor will need to balance pain relief with potential side effects.
Common Types of Muscle Relaxants
Here are some common muscle relaxants you might encounter on a prescription pad:
- Cyclobenzaprine (Flexeril): Popular for nighttime use in bruxism-related pain. Usual dose is 5–10 mg before bed.
- Tizanidine (Zanaflex): Shorter half-life, which can help avoid next-day brain fog.
- Baclofen: Sometimes paired with NSAIDs for inflammatory cases.
- Carisoprodol: Effective but carries a dependency risk, so it’s avoided for long-term therapy.
When traditional options fall short, injectables like OnabotulinumtoxinA (BoNT-A) can be considered. A 2025 cohort study by Henien et al. found a 45 percent pain reduction three months post-injection, though these treatments can be expensive and require repeat sessions. For a detailed comparison, our article on bruxism mouth guards vs. muscle relaxants offers insights into managing TMJ pain effectively.
Comparing TMJ Medication Options
Choosing a drug isn't straightforward. Let's compare muscle relaxants with other TMJ medications—NSAIDs, antidepressants, anticonvulsants, and local anesthetic injections—to see where each stands out or falls short.
Muscle Relaxants vs. Other Medications
An umbrella review by Christidis et al., 2024, ranks first-line drug classes for TMD based on pain reduction, functional improvement, and side effects:
- NSAIDs (ibuprofen, naproxen): Effective for acute inflammation but can irritate the stomach with prolonged use.
- Muscle Relaxants: Ideal for nocturnal bruxism or myofascial spasm, with less gastrointestinal upset, but they can cause drowsiness.
- Antidepressants (amitriptyline, duloxetine): Useful for chronic centralized pain, though side effects like dry mouth and weight gain may occur.
- Anticonvulsants (gabapentin): Target nerve-related pain but require slow titration.
- Opioids: Generally discouraged for TMD due to dependency risks.
A 2025 randomized controlled trial by Gurudut et al. compared muscle relaxants with soft tissue manipulation. Both groups improved, but medication provided faster short-term relief, while manual therapy offered longer-lasting functional gains at 12 weeks. For insights into manual therapy, see our article on the role of physical therapy in TMJ pain management.
Pros and Cons
- Pros of Muscle Relaxants:
- Reduce nocturnal clenching intensity
- Lower acute muscle pain quickly (often within a week)
- Can be taken as needed to avoid daily side effects
- Cons:
- Drowsiness, especially with cyclobenzaprine and baclofen
- Potential interactions with alcohol or CNS depressants
- Not ideal for those who operate heavy machinery early in the morning
Use the pros-cons grid like a dating profile—know what you can tolerate before committing.

Non-Pharmacological Alternatives for TMJ Pain
Drugs are useful but not the whole story. Combining medication with non-pharmacological strategies can enhance results. The same 2025 review by Jogna et al. emphasizes a multimodal approach for chronic TMD, and the Gurudut RCT supports this.
Physical Therapy
Targeted jaw stretches, trigger-point massage, and posture exercises can relax overworked muscles, enhancing medication effectiveness. Key exercises include:
- Isometric Jaw Exercises: Press your tongue to the roof of the mouth and gently open the jaw halfway, holding for five seconds.
- Chin Tucks: Retract your chin toward your neck to strengthen deep neck flexors supporting the jaw.
- Masseter Massage: Use two fingers to knead cheek muscles in slow circles.
In the Gurudut trial, soft tissue work combined with home exercises reduced pain scores by 50 percent at eight weeks—comparable to muscle relaxants but without morning grogginess. For passive therapy fans, dry needling shows promise as an innovative approach for TMJ pain relief.
Lifestyle Changes
- Sleep Hygiene: Poor sleep worsens bruxism. Set a regular bedtime and avoid caffeine after 2 p.m. A 2024 review by Leung et al. links disrupted sleep to pediatric bruxism, and adults are no different. For more, read about how sleep positions affect bruxism.
- Stress Management: Mindfulness and cognitive behavioral therapy (CBT) reduce grinding by addressing the stress-clench reflex. Our article on mindfulness techniques can offer practical stress-relief strategies.
- Diet Tweaks: Temporarily avoid chewy foods like bagels and gum that strain the jaw.
- Posture Improvements: Ergonomic desks and screen adjustments reduce neck strain and TMJ tension.
- Night Guards: Custom mouth guards from a dentist cushion grinding forces and work well with bedtime muscle relaxants.
Combining these habits with medication offers both quick relief and long-term protection against flare-ups. For those seeking dietary adjustments, explore our article on diet's role in managing bruxism.
Case Studies and Real-World Applications
Theory is great, but real-life experiences tell the real story. Here are examples from research and clinical practice showing how muscle relaxants work in daily life.
Patient Experiences
- Case 1: The Night-Shift Nurse
Maria, 34, worked rotating shifts and woke up with jaw pain daily. After a sleep study identified severe bruxism, her physician started cyclobenzaprine 5 mg at bedtime and recommended a night guard. Within two weeks, her pain dropped from 7 to 3 on the visual analog scale (VAS). She felt groggy the first few mornings but adjusted by taking the pill an hour earlier. - Case 2: The Graduate Student Gamer
Leo, 26, wore through three mouth guards during finals week. His dentist added tizanidine 2 mg at night and referred him for physiotherapy. After eight sessions and medication, his VAS score dropped by 60 percent, and he could yawn without locking his jaw.
Clinical Outcomes
A 2025 cohort study by Henien et al. tracked 48 TMD patients receiving BoNT-A injections in the masseter and temporalis muscles. Pain scores significantly decreased at one month, and the effect lasted up to four months before tapering. A parallel animal model by Kim et al., 2025, supported these findings, showing reduced inflammatory markers after injection.
For oral meds, Patel and Ouanounou’s 2026 review found that cyclobenzaprine users experienced an average 2 mm increase in painless mouth opening—small in measurement but significant when biting into a sandwich without wincing.
The takeaway: muscle relaxants are not magic bullets, but when combined with lifestyle changes and mechanical aids, they improve outcomes.
Future Directions in TMJ Treatment
Innovation continues, especially where pain management meets biotech. Here's a look at what might be next in TMJ treatment.
Emerging Research
Researchers are exploring molecular strategies to enhance drug delivery. A preclinical study by Yuan et al., 2025, found that strontium-alix interactions improve exosomal microRNA loading in synovial mesenchymal stem cells, potentially aiding cartilage regeneration. While early, such biologics could support muscle relaxants by repairing the joint while calming muscles.
On the pharmacology front, extended-release tizanidine formulations aim to stabilize plasma levels, reducing rebound tightness without increasing sedation risk. Phase III trials are expected soon.
Potential Breakthroughs
- Personalized Medicine: Genotyping for cytochrome P450 enzymes could predict cyclobenzaprine metabolism rates, allowing tailored dosages to avoid excessive sedation.
- Wearable Tech: Biofeedback headbands that alert users to clenching are in prototype testing, with early data indicating a 40 percent reduction in daytime bruxism episodes.
- Combination Patches: Transdermal patches releasing low-dose tizanidine and NSAIDs offer steady relief without pills. Animal models show promise.
- Virtual Reality (VR) Rehab: Gamified jaw exercises in VR can improve compliance, especially for tech-savvy teens.
These advancements could complement existing muscle relaxants, further personalizing TMJ treatment.
Conclusion
So, do muscle relaxants deserve a place in your TMJ treatment plan? The evidence supports their use, particularly for bruxism or muscle spasm-driven pain. Reviews by Patel and Ouanounou and Christidis et al. confirm significant pain reduction and improved mouth opening. Remember, they work best with non-drug strategies like physical therapy, stress management, and night guards. Discuss dosing, timing, and potential interactions with your healthcare provider—because the only thing worse than jaw pain is dozing off at work after an oversized cyclobenzaprine dose.
Armed with clinical data and a practical approach, you can make informed decisions rather than relying on chance. Your jaw, sleep, and well-being will thank you.