Advanced Clinical Solutions for Bruxism: From Botox to Surgery
Explore advanced bruxism treatments, including Botox and surgical options.

You wake up with a sore jaw, a dull headache, and your partner swears you sound like a wood chipper at night. That symphony of grinding and clenching is called bruxism. It's more common and treatable than most people think. Thanks to a wave of clinical research, you have more options than ever, from time-tested mouthguards to Botox and even surgical fixes for the toughest cases.
This article walks you through those options in plain language. We will lean on recent systematic reviews, pilot studies, and guidelines from reputable organizations so you can sort hype from help before you talk with your dentist or sleep specialist.
Understanding Bruxism and Its Impacts
Bruxism is the involuntary grinding, clenching, or gnashing of teeth that happens while you sleep or, less commonly, when you are awake. Somewhere between 10 and 15 percent of adults do it often enough to need treatment, according to the American Dental Association. It's not just a noisy habit. Over time it can shorten or crack teeth, inflame the temporomandibular joint (TMJ), trigger migraines, and chew through your quality of life.
Although bruxism peaks in the 20-to-40 age range, it can start as early as childhood and persist into older adulthood. Pediatric dentists now screen routinely because early intervention can prevent malocclusion later in life. Clinicians also note a circadian rhythm to the condition. Episodes cluster in the first two rapid eye movement (REM) cycles when muscle tone is highest. In other words, the grinding is most ferocious before you even reach your deepest sleep.
Signs and Symptoms
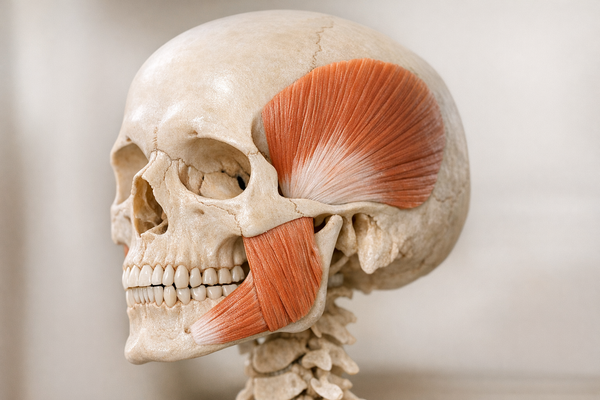
You might notice flattened tooth surfaces, chipped enamel, or sudden tooth sensitivity. Morning jaw stiffness, earaches without an ear infection, and tension headaches also point to nocturnal grinding. Bed partners often pick up the problem first because they hear the sounds that you sleep right through. A useful red flag is jaw muscle hypertrophy—your masseters can bulk up if they are flexing all night.
Less obvious clues include scalloped tongue edges, small “notches” at the gum line from flexing teeth, and a clicking or popping TMJ when you yawn. During dental exams, your provider may apply articulating paper to reveal shiny wear facets invisible to the naked eye—an objective sign that the enamel has been under siege. For more on identifying early signs, explore Recognizing Bruxism Symptoms.
Causes and Risk Factors
Why do you grind? Stress tops the list, but crooked bites, missing teeth, certain medications, and sleep disorders like obstructive sleep apnea play leading roles. A review by van Looij et al. found that apnea patients face roughly double the bruxism risk. Genetics is another wildcard: if both your parents gnash, odds are you might, too. Finally, lifestyle habits—think caffeine overload or late-night alcohol—can crank up muscle activity during REM sleep. For more insights, consider reading Can Stress Cause Bruxism?
Prescription drugs deserve a special call-out. Selective serotonin reuptake inhibitors (SSRIs), amphetamine-based ADHD medications, and even some over-the-counter decongestants have been linked to increased jaw activity. If your grinding started after a medication change, flag it for your prescriber. An alternative formulation may calm your nocturnal muscles. For more information on medication-related bruxism, check Adderall and Teeth Grinding.
Unmanaged bruxism snowballs. A meta-analysis by Assiri and colleagues showed that people with moderate to severe grinding lose an average of 1.5 mm of tooth height every decade. That's like sanding down a tooth with each passing birthday.
Occlusal Splints: Traditional yet Effective
The go-to treatment you have probably heard of is the occlusal splint—also known as a night guard or bite plate. It is a removable acrylic or thermoplastic device that fits over your upper or lower teeth, redistributing bite forces and cushioning enamel. For a detailed guide on choosing the right type, visit How to Choose the Right Bruxism Treatment.
Types of Splints
Classic hard acrylic guards are still popular, but soft EVA (ethylene-vinyl acetate) versions feel more forgiving. Dual-laminate guards combine a hard outer shell with a soft inner layer. Then there are anterior deprogrammers, which cover only the front teeth to limit clenching intensity.
Innovation has arrived via 3D printing. A review by Šimunović et al. reported that printed splints can be fabricated in a single dental visit with micron-level accuracy, sparing you the gag-worthy impression tray. You can even tweak occlusion digitally before the printer starts.
Over-the-counter “boil-and-bite” guards exist, but they often fit poorly and may shift teeth over time. If budget is tight, consider at-home impression kits reviewed remotely by a dentist. They land in a middle ground between generic and fully custom devices. For comparisons of different mouth guard types, see Night Guard Comparison: Custom vs. Over-the-Counter.
Efficacy and Limitations
Do they work? Absolutely—within limits. A head-to-head meta-analysis comparing splints with Botox by Aldosari et al. showed splints dropped self-reported pain scores by roughly 40 percent and cut enamel wear progression in half over six months. They are also non-invasive and reversible. Yet splints are only as good as your bedtime discipline. Forget to pop it in and you're back at square one.
Practical tip: store the guard in a vented case with a splash of chlorhexidine rinse once a week to deter funk-producing bacteria. Consider setting a phone alarm an hour before bedtime; compliance-tracking apps that pair with Bluetooth cases are now entering the market, turning your night guard into a miniature “smart” device. For cleaning tips, check How to Clean a Night Guard.
They can fracture, feel bulky, or shift your bite if adjusted poorly. Plus, they do not treat underlying muscle hyperactivity; they merely shield teeth from the fallout. Splints earn their spot as first-line therapy, but they are not magic.

Botox for Bruxism: A Modern Approach
Botulinum toxin type A—Botox—has moved from smoothing wrinkles to calming overworked jaw muscles. When injected into the masseter and sometimes the temporalis, Botox blocks acetylcholine release, causing temporary muscle relaxation. For more on this treatment, explore Botox for Bruxism or Teeth Grinding.
Mechanism of Action
Think of Botox as a dimmer switch. Instead of paralyzing the muscle, therapeutic doses temper its peak strength. Less clamping force means less grinding noise, fewer fractures, and a break for your TMJ.
Clinical Evidence
The literature is positive. A systematic review by Yacoub et al. pooled data from 11 controlled trials and found Botox reduced nocturnal electromyographic (EMG) activity by 28-50 percent over three months. Pain and disability scores improved two to three times faster than with splints alone.
Real-world dosing generally ranges from 20 to 30 units per masseter, yet some high-intensity grinders need up to 50 units split across multiple injection points. Expect mild chewing fatigue for a week—a great excuse to lean on smoothies and soft foods while the toxin settles.
Cost and upkeep matter. Injections run every three to four months because new nerve endings sprout. Over time that can outprice a one-time splint. On the upside, Botox also softens the square-jaw look from hypertrophic masseters, a cosmetic perk for some.
Side effects are uncommon but real: transient chewing fatigue, smile asymmetry if the dose wanders, and rare allergic reactions. Choose an injector who treats bruxism regularly, not just crow’s-feet.
How does it stack up against splints? Aldosari’s meta-analysis again showed Botox outperformed splints on pain reduction at three months but evened out by the one-year mark. That suggests Botox shines when you need quick relief, while splints win on long-term cost and simplicity.
If you are juggling both, no worries. Studies like Coelho et al. endorse combination therapy: wear a night guard for mechanical protection and top off with Botox for muscle calm.
Innovative Therapies on the Horizon
The treatment toolbox is expanding beyond plastics and toxins. Researchers are tinkering with electrical stimulation, biofeedback, and even smartphone-guided coaching. None are ready to dethrone established therapies yet, but they are worth watching.
TENS Therapy
Transcutaneous electrical nerve stimulation (TENS) is better known for back pain, yet pilot studies suggest it can dial down jaw muscle hyperactivity. A quirky but intriguing study by Aydoğan et al. strapped pencil-sized electrodes onto the masseter. After four weeks, participants reported a 30 percent drop in tinnitus linked to bruxism and a parallel decline in grinding frequency on EMG logs.
How does it work? Mild electrical pulses fatigue the muscle fibers and may neuro-modulate pain pathways. The therapy is non-invasive and home-friendly, but long-term data are thin, and optimal dosing is guesswork for now. Physical therapists trained in orofacial pain can help you fine-tune pad placement and intensity so that the gadget doesn’t gather dust. For more information on non-invasive treatments, see Natural Bruxism Solutions.
Emerging Technologies
- Bite-sensor wearables: Think fitness tracker for your jaw. Pressure sensors in a slim mouthpiece record clench events and vibrate to nudge you out of micro-grinds. Early prototypes are in clinical trials cited by the National Institute of Dental and Craniofacial Research.
- Biofeedback apps: Smartphone microphones detect grinding sounds and trigger auditory cues. The approach is cheap but plagued by false alarms, so researchers are refining algorithms before widespread release. For insights on biofeedback, check Understanding Biofeedback Devices for Effective Bruxism Management.
- Pharmacologic molecules: Low-dose muscle relaxants or dopamine modulators are being explored, but side-effect profiles keep enthusiasm cautious.
Many of these ideas piggyback on digital dentistry advancements listed in the 3D splints review by Šimunović et al. The moral: keep an eye on this space if you are an early adopter.
Surgical Interventions: A Last Resort
Most grinders never need a scalpel, but there are rare situations where surgery makes sense—severe TMJ damage, congenital jaw misalignment, or catastrophic tooth wear defying conservative care.
When Surgery is Necessary
Your dentist or maxillofacial surgeon may order 3D scans and motion studies before even floating the idea. Candidates often fail at least six months of splint, Botox, and behavioral therapy. Chronic pain, locked jaws, or inability to chew may tip the scales toward surgery.
Insurance coverage is patchy; some carriers classify bruxism as “behavioral” rather than medical, so request a pre-authorization letter detailing functional impairment. A second opinion from a university-based clinic can also clarify whether invasive treatment is truly warranted.
Types of Surgical Options
- Arthrocentesis or arthroscopy: Minimally invasive flushing of the TMJ to remove inflammatory debris and free a stuck disc. For more on TMJ relief, visit Exploring New TMJ Treatments.
- Mandibular osteotomy: Repositions an underbite or cross-bite that fuels abnormal muscle pull.
- Subperiosteal implantation or reconstruction: For jaws wrecked by wear, titanium frameworks rebuild lost bone, as reported in a complication-management paper by Mommaerts.
Risks include infection, nerve injury, and the dreaded relapse if underlying habits persist. Recovery spans weeks to months with liquid diets and physiotherapy. Hence surgery is labeled “last resort,” not because it never works, but because the price—biological and financial—is steep.

Comparative Analysis of Treatment Outcomes
Let’s pit the options head-to-head so you can weigh convenience, cost, and effectiveness.
Pros and Cons of Each Approach
- Occlusal splints
Pros: Non-invasive, custom fit, one-time cost, backed by decades of data.
Cons: Compliance-dependent, can break or warp, do not relax muscles.
Evidence: 40 percent pain reduction in Aldosari's study. - Botox injections
Pros: Rapid symptom relief, shrinks bulky jaw muscles, can pair with splints.
Cons: Needs repeat dosing, higher cumulative cost, mild side effects possible.
Evidence: 28-50 percent EMG drop in Yacoub's study. - TENS and emerging tech
Pros: Non-pharmacologic, DIY potential, minimal systemic risk.
Cons: Limited long-term data, gadget costs, user learning curve.
Evidence: 30 percent symptom drop in Aydoğan's study. - Surgery
Pros: Definitive fix for structural issues, can restore function when all else fails.
Cons: Invasive, expensive, recovery time, complication risk.
Evidence: Case series reported predictable outcomes when criteria met, per Mommaerts.
A broader umbrella review by Assiri et al. concluded that blended approaches—splint plus behavioral therapy, Botox plus splint, or splint followed by corrective surgery—yield the highest patient-reported satisfaction. Meanwhile, a clinical protocol paper on interceptive tooth-wear management by Dietschi suggests early intervention is cheaper and easier than chasing down late-stage damage. For managing stress-induced bruxism, see How to Stop Clenching Your Teeth at Night.
Conclusion: Finding the Right Solution for You
Bruxism is a multifaceted beast, but the toolbox to tame it has never been better stocked. Occlusal splints remain the sturdy workhorse, Botox offers fast muscle relief, innovative gadgets deliver promising DIY tweaks, and surgery stands guard for the outliers who truly need it.
Your best first step is a frank chat with a dental or sleep professional. Bring a list of symptoms, maybe a phone recording of your nighttime grinding, and questions about the options covered here. Toss in a review of your current medications—sometimes a simple switch can lower the stakes dramatically. Together you can map a plan that aligns with your budget, comfort level, and clinical severity. With evidence piling up and technology advancing, you can finally retire that wood-chipper soundtrack and give your teeth the peaceful night they deserve.