Understanding Jaw Pain: Is Anxiety the Culprit?
Explore jaw pain causes and differentiate anxiety from other issues in this detailed guide.
Jaw pain can disrupt your day, whether it's a dull ache or a sharp stab. You might wonder if it's a dental problem, muscle tension, or something mental. Research suggests anxiety often plays a key role, but it's not alone. This guide explores the science to help you determine when stress is the cause and when to seek other help.
This evidence-based guide minimizes jargon and answers questions you might not know to ask. Ready to explore the facts? Let's dive in.
Understanding Jaw Pain Anatomy
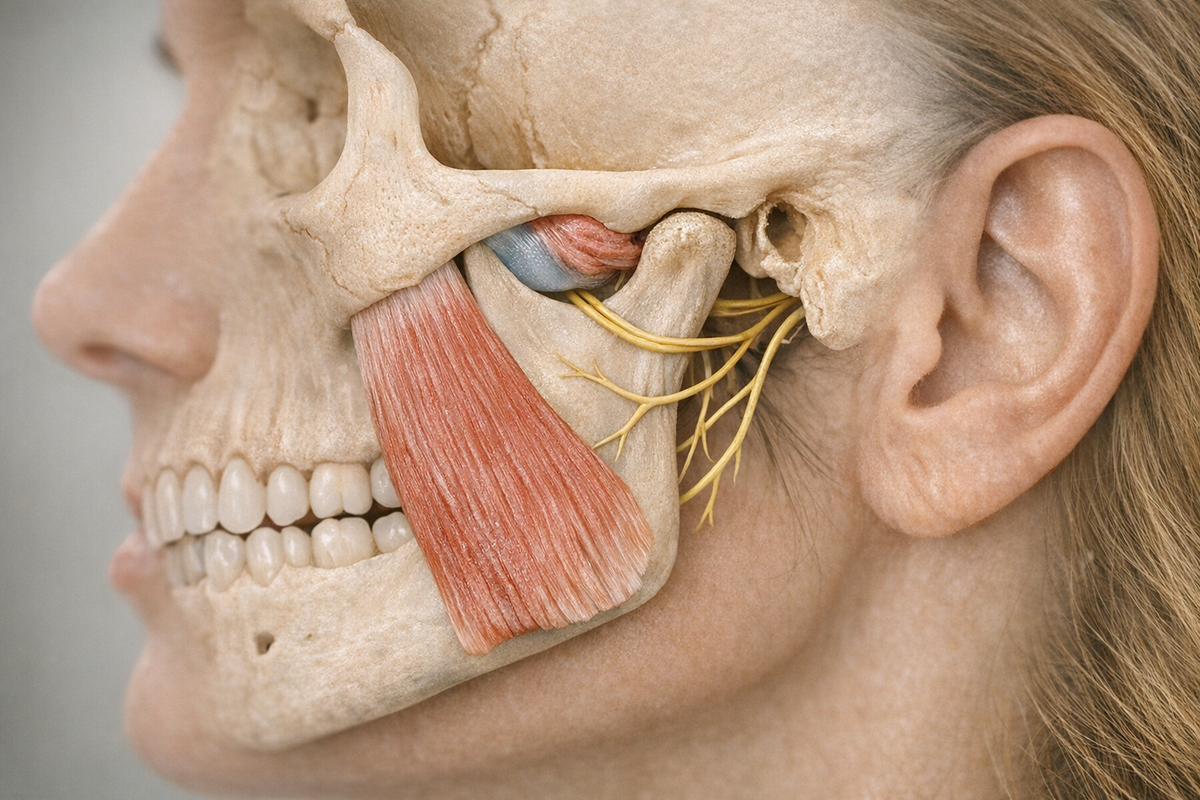
Your jaw is where bones, muscles, nerves, and cartilage meet. The temporomandibular joint (TMJ) is a sliding hinge that connects your lower jawbone (mandible) to the temporal bone of your skull. Each TMJ has a small disc that allows smooth movement. The masseter and temporalis muscles handle chewing, while smaller muscles aid in speech and facial expression.
When these structures malfunction, you might feel:
- Aching in front of the ears
- Popping or clicking when biting
- Locking that restricts mouth opening
- Referred pain in the temple, neck, or shoulder
- Headaches similar to tension or migraines
These symptoms can disrupt daily life—chewing becomes cautious, talking effortful, and sleep interrupted by nocturnal clenching. A 2025 literature review by Raciti et al. notes the overlap of jaw pain with ear pain and facial neuralgia, causing many to bounce between dentists, ENT doctors, and neurologists before finding the right diagnosis.
Why such confusion? The mandibular branch of the trigeminal nerve carries both sensory and motor fibers, so irritation can produce multiple pain signals. Additionally, jaw muscles share space with facial muscles, which respond to emotional states. When anxiety increases, these muscles tense—more on that soon.
In summary, understanding the components helps identify the type of jaw pain—whether mechanical, inflammatory, neuropathic, or anxiety-related.

Connecting Anxiety and Jaw Tension
Anxiety-Induced Jaw Pain
Anxiety affects your entire body. When you perceive a threat, your brain activates the sympathetic nervous system. Muscles tighten, breathing quickens, and your jaw may clamp shut. A 2026 study by Chang and Cho used functional MRI during anxiety-inducing storytelling and found stronger connectivity among three brain networks: the salience network (which detects danger), the default mode network (which generates internal narratives), and the executive control network (which plans responses). This explains why racing thoughts can lead to clenched teeth: the brain's worry circuits communicate with the motor areas controlling jaw muscles.
Persistent activation is problematic. When your salience network is constantly alert, the masseter and temporalis muscles cannot relax. Micro-contractions can form trigger points—small knots that shorten muscle fibers, reduce blood flow, and cause pain. Over time, habitual clenching may alter jaw mechanics, potentially leading to disc displacement or TMJ arthritis.
Impact of Oral Behaviors
Oral behaviors include actions like nail biting, gum chewing, pencil gnawing, and teeth clenching. A 2025 study by Michelotti et al. found that oral behaviors mediated the link between anxiety and painful TMJ disorders. Anxiety alone did not predict jaw pain unless people also clenched or ground their teeth. This is promising because behaviors can be changed. However, many are unaware of these behaviors, especially when they occur during sleep or while focused on a screen.
Key takeaways:
- Anxiety primes your brain to tense jaw muscles before you feel stressed.
- Habitual oral actions turn short-term tension into chronic pain.
- Tracking habits with apps or sticky notes can increase awareness and disrupt the cycle.
Stress and Awake Bruxism
Bruxism refers to grinding or clenching. While sleep bruxism is often discussed, awake bruxism is equally damaging. It manifests as jaw tightening during various activities.
An observational study by Emodi-Perlman et al. in 2025 tracked working adults for a year and found stress spikes predicted increases in awake bruxism. Participants wore EMG sensors on their masseter muscles, capturing clenching episodes that might otherwise go unnoticed. Prolonged stress increased baseline muscle tension, turning occasional clenchers into habitual ones.
Long-term stress affects jaw health:
- Mitochondrial fatigue: Stressed muscles deplete ATP, leading to fatigue and soreness.
- Cytokine release: Chronic stress raises inflammatory markers like IL-6, sensitizing pain receptors.
- Hormonal shifts: Elevated cortisol can thin cartilage, making the TMJ disc more prone to wear.
Can supplements help? Animal data suggest so. A mouse study by Lee et al. in 2025 showed that Withania somnifera (ashwagandha) reduced anxiety-like behavior and moderated hippocampal changes after stress. While mice are not humans, early trials suggest the herb may lower perceived stress and clenching frequency. Consult your healthcare provider before starting any herbal routine.
Meanwhile, the American Psychological Association suggests proven stress-busters like aerobic exercise, scheduled downtime, and social connection. These reduce physiological arousal that feeds awake bruxism.

Temporomandibular Disorders: More than Anxiety
Biopsychosocial Factors
Temporomandibular disorders (TMDs) include issues affecting the jaw joint or chewing muscles. Anxiety is a factor, but genetics, hormones, posture, sleep apnea, and systemic diseases like rheumatoid arthritis also contribute. The National Institute of Dental and Craniofacial Research labels TMDs as "multifactorial" on its official page.
A 2025 paper by Kuć et al. highlights oxidative imbalance as a factor. Patients with myofascial TMD showed elevated malondialdehyde (a lipid peroxidation marker) and reduced antioxidant enzymes. Simply put, their jaw muscles had more "rust" and fewer "rust removers," making them more prone to fatigue and pain. High anxiety plus oxidative stress produced the worst jaw limitations, a combination that standard dental guards couldn't fix alone.
Clinical Symptoms
How do multifactorial causes manifest? Here are common symptom clusters:
- Myofascial pain: Dull, aching soreness worsening with use
- Internal derangement: Clicking or popping from disc displacement
- Arthralgia: Sharp, localized joint pain worsened by chewing
- Headache overlap: Pain radiating into temples or behind the eyes
- Ear-related symptoms: Ringing, fullness, or mild hearing changes without infection
A 2025 literature review by Raciti et al. argues that no single symptom or test can confirm TMD, as it often coexists with conditions like fibromyalgia or migraine. This complexity explains why people with similar MRI findings may report different pain levels—psychological context matters.
Takeaway: TMD involves many factors; anxiety is significant but not exclusive.
Distinguishing Anxiety from Other Causes
Psychological vs. Physical Disorders
Jaw pain is complex, so distinguishing anxiety-related discomfort from organic disease is crucial. Begin with a structured history:
- When does pain occur—during stressful tasks or while eating?
- Does relaxation or painkillers improve the pain?
- Are there systemic symptoms like fever, numbness, or swelling?
Next, consider a clinical exam. Dentists trained in orofacial pain will palpate jaw muscles, check range of motion, and listen for joint sounds. Surface electromyography may be used to measure muscle activity. If nerve involvement is suspected, neurophysiological testing can rule out rare conditions like trigeminal neuralgia.
On the psychological side, tools like the Hamilton Anxiety Rating Scale can determine if anxiety scores track with pain spikes. If high anxiety coincides with minimal mechanical issues, anxiety-dominant jaw pain is likely.
Case Studies and Examples
1. Case A: A 28-year-old programmer reports jaw tightness during coding marathons. No clicking, full range of motion. EMG shows elevated masseter activity only while working. Anxiety inventory is high. Diagnosis: stress-induced awake bruxism.
2. Case B: A 45-year-old teacher wakes up with right-sided jaw locking. CT scan reveals osteoarthritic changes. Anxiety scores are normal. Treatment targets TMJ degeneration, not stress.
3. Case C: A 32-year-old with obsessive-compulsive disorder develops severe myofascial pain. A 2025 case series by Pourshahidi et al. shows how psychiatric comorbidity can amplify pain perception, even with mild structural findings.
Even controversial topics arise. Neuralgia-Inducing Cavitational Osteonecrosis (NICO) is debated. A critical review by Keith, 2025 notes inconsistent evidence and recommends ruling out more common causes first.
Treatment and Management Strategies
Reducing Stress
If anxiety is the main driver, calm the nervous system first. Effective methods include:
- Mindful breathing: Inhale for four counts, exhale for six. Repeat for five minutes twice daily.
- Progressive muscle relaxation: Tense then relax facial muscles from forehead to chin.
- Cognitive behavioral therapy (CBT): Targets thought patterns that trigger clenching.
- Adaptogens: Withania somnifera may lower cortisol and muscle tension.
- Biofeedback apps: EMG graphs teach you to spot and stop clenching.
The American Psychological Association lists these techniques on its stress management page, emphasizing consistency over intensity.
Medical and Dental Interventions
When structural problems are present, a broader toolkit is needed.
- Occlusal splints: Night guards cushion teeth and reduce grinding forces. They don't cure anxiety but protect enamel while working on stress.
- Physical therapy: Jaw stretching and posture training ease muscle imbalances.
- Anti-inflammatory diet: High in omega-3s and antioxidants to counter oxidative stress highlighted by Kuć et al.
- Medications: Short-term NSAIDs for acute flare-ups; low-dose tricyclics for neuropathic components.
- Botulinum toxin: Injections into overactive masseter muscles can break the clenching cycle for 3-4 months. Use with caution and expert guidance.
- Surgery: Reserved for severe disc displacement or degenerative joint disease when all else fails, per Mayo Clinic guidelines on TMJ disorders.
Combination care works best. For example, a patient might wear a night guard to limit physical damage, practice CBT to reduce worry, and follow an anti-inflammatory diet to tackle oxidative stress. Over time, these combined efforts lead to pain reduction.
Conclusion
Jaw pain is rarely a one-note problem. Anxiety, stress, mechanical wear, and biochemical changes all contribute. Research—from the triple network fMRI study by Chang and Cho to oxidative stress findings by Kuć et al.—shows the link between mind and body at the jaw joint. Separating anxiety-driven tension from structural disorders requires a careful history, targeted exams, and sometimes specialized tests.
The good news is that treatment options are expanding. Mindfulness, therapy, and lifestyle tweaks calm the brain circuits that tighten your jaw, while dental appliances and physical therapy protect and heal the tissues. The key is matching the solution to the root cause. When in doubt, consult a dentist or orofacial pain specialist to help sort psychological triggers from mechanical ones. Your jaw—and your sanity—will thank you.


