Could Your Sleeping Position Be Causing Jaw Pain? Understanding the Connection
Explore how your sleeping position might cause jaw pain and learn solutions.

You wake up, stretch, and immediately notice a dull ache on one side of your jaw. It might pop when you yawn, or feel tight when you try to bite into breakfast. If that sounds familiar, you're in crowded company. Morning jaw pain is so common that dentists have nicknamed it “alarm-clock jaw.” The question is why it happens. Research suggests an unexpected suspect right under your pillow—your favorite sleeping position.
Below, we explore how your sleeping position might strain jaw joints, affect muscles, and interact with conditions like bruxism and obstructive sleep apnea (OSA). You'll also find strategies to reduce the pain before it ruins another morning.
Understanding Jaw Pain and Sleep
Morning jaw pain is more than an annoying kink. In large surveys, up to one in five adults report jaw discomfort that peaks right after waking. Clinicians notice a pattern: pain often sits on one side, worsens when you open wide, and eases after a hot shower or a few hours of activity. While tooth decay and gum disease can hurt, they usually throb all day. Jaw pain that improves midday suggests something happens during sleep.
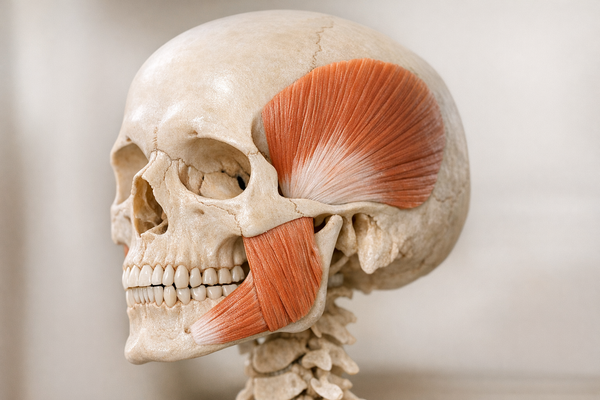
So, what goes on at night? A review of obstructive sleep apnea cases by van Looij and colleagues noted that nearly half of patients with apnea also reported morning jaw soreness. Another clue came from Kuang, Lobbezoo, and Li’s investigation into bruxism patterns. They found that people who favored certain sleep positions—especially side-lying with the jaw pressed into the pillow—showed higher muscle activity in the masseter, the main chewing muscle.
These studies suggest a two-part story. First, the jaw might be squeezed by pressure from your pillow or mattress. Second, the body may respond with micro-movements or clenching to keep the airway open, especially if OSA is present. Over a night, those contractions can irritate the temporomandibular joint (TMJ) and muscles. Come sunrise, you feel the aftermath as stiffness, tenderness, or a clicking joint.
Other factors like stress, caffeine, and misaligned teeth can increase the odds of grinding or clenching. However, even if you tick every box on the risk-factor list, where you rest your head remains a key modifiable trigger. For more insights, explore how sleep positions can cause jaw pain and bruxism.
The Science of Sleep Positions and Jaw Pain
Sleep researchers divide body positioning into three main camps: supine (on your back), prone (on your stomach), and lateral (on your side). Each creates unique mechanical forces on the jaw.
Back sleeping usually lets the jaw hang open due to gravity. For some, this can narrow the airway and lead to snoring or apnea events. The brain reacts by activating jaw muscles to pull the mandible forward, which can become a nocturnal workout. Side sleeping shifts the lower jaw sideways, especially if you bury a cheek in a thick pillow, pressing the TMJ. Stomach sleeping twists the neck and jaw far to one side for hours, creating an uneven load that often appears as one-sided pain in the morning.
In a cohort of OSA patients, Kuang et al. recorded EMG data and confirmed that lateral positions increased masseter muscle activity compared with back sleeping. Their conclusion: the mechanical compression of the jaw in side sleepers may maintain or aggravate bruxism episodes. Parallel work on low-Fowler positioning—back sleeping with the torso slightly elevated—showed that muscle bursts dropped in frequency, hinting that a small tilt could be protective (Zhong et al.).
OSA turns this positional story into high drama. When the airway collapses during REM, negative pressure pulls the jaw backward. Clenching or protruding the mandible helps reopen the airway. If you're on your back, gravity compounds the obstruction. Side sleeping often improves airflow, but if your pillow is too firm, you trade airway relief for mechanical jaw strain. This explains why OSA patients frequently juggle both respiratory and TMJ complaints (van Looij et al.).
Common Sleep Positions and Their Impact
- Supine (back): Lower jaw drops back, possibly triggering airway collapse and reflex clenching. Proper pillow elevation can offset this.
- Lateral (side): Airway is usually clearer, but the downward cheek pushes the condyle into the socket, straining one TMJ.
- Prone (stomach): Requires head rotation to breathe, twisting the neck and jaw, often leading to asymmetrical morning pain.
- Low Fowler (30-degree back incline): Shown to reduce bruxism bursts in controlled trials, blending airway patency with gentle jaw support.
The takeaway: No single position is “perfect.” Instead, matching the right pillow height, mattress firmness, and slight trunk angle can lower stress on both airway and jaw. For those dealing with bruxism and jaw pain, these adjustments can be particularly beneficial.

Bruxism and Jaw Pain Connection
Bruxism refers to teeth grinding or clenching. It comes in two main forms: awake bruxism (daytime) and sleep bruxism (nighttime). The American Dental Association estimates that 10 percent of adults grind their teeth at night. Symptoms include flattened tooth surfaces, tooth sensitivity, and morning jaw pain.
Why does grinding often hurt only one side? Picture clenching harder on the pillow side if you sleep laterally. That unilateral load can irritate just one TMJ, causing pain when you try to open wide on awakening. In a randomized study by Karabicak Gul and colleagues, participants used jaw exercises, combined jaw-and-posture exercises, or a standard occlusal splint. The combined exercise group showed the biggest drop in morning pain scores, suggesting that muscular conditioning and posture retraining can blunt the grinding-pain cycle.
Treatment research spans splints, Botox, behavioral coaching, and novel pillow designs. A pilot trial compared Botox injections with soft thermoformed occlusal splints in moderate sleep apnea sufferers who also had nocturnal bruxism (Taalat Gavrilă et al.). Both groups reported satisfaction, yet splints slightly outperformed injections for pain relief over three months. This aligns with dental advice: keep the bite balanced and cushion tooth-to-tooth impact first, then layer on muscle interventions if needed. For more on advanced treatment options, explore clinical solutions for bruxism.
For day-to-day management, the ADA’s bruxism page notes that limiting caffeine after lunch, cutting back on alcohol, and practicing jaw relaxation drills before bed reduce nocturnal muscle activity. More tech-savvy approaches include biofeedback devices that vibrate when they sense grinding, effectively nudging you to shift position mid-sleep.
Still, none of those tactics matter much if you sleep with your jaw in a half-Nelson. Position remains the silent enabler. Change the posture, change the pressure, and bruxism often calms down too.
Temporomandibular Disorders (TMD) and Sleep
Temporomandibular disorders are a group of joint and muscle problems that intersect dentistry, neurology, and psychology. Symptoms include jaw clicking, limited opening, ear pain, and headaches starting near the temples. According to the National Institute of Dental and Craniofacial Research, up to 12 percent of the US population deals with TMD at any given time.
How does sleep position fit in? TMD pain correlates strongly with oral behaviors (clenching, gum chewing) and poor sleep quality. An observational study of TMD patients by Yap, Zheng, and Luo found that those who napped or slept in awkward positions during the day recorded higher jaw disability scores. Similarly, Tian et al. surveyed a general population sample and found that side sleepers who propped the jaw on a hand or arm during slumber reported more TMD symptoms than neutral sleepers.
Chronic pain meta-analyses support the posture link. A network review in BMJ compared 54 randomized trials on TMD pain management and flagged ergonomic education—including sleep position coaching—as a low-cost, moderate-benefit strategy (Yao Liang et al.).
Standard treatments follow a stepped model:
- Self-care: Soft diet, warm compresses, sleep hygiene.
- Conservative therapy: Occlusal splints, physical therapy, and cognitive behavioral therapy for pain coping.
- Invasive options: Botox, injections, or surgery, reserved for stubborn cases.
Where you lay your head belongs solidly in step one. A smaller, contoured pillow that maintains neutral cervical alignment can unload the TMJ, while a side-sleep wedge minimizes face-down pressure. Cleveland Clinic’s online guide to jaw pain underscores that repositioning may take a week of trial-and-error but often yields noticeable relief. For more tips on managing jaw tension, consider jaw relaxation techniques for stressed professionals.

Lifestyle Adjustments to Alleviate Jaw Pain
You don't have to overhaul your life or buy a robot pillow to see progress. Small habit tweaks add up.
Practical Tips for Better Sleep
- Audit your pillow. Too high or too flat puts the neck out of sync with the jaw. Aim for a pillow that keeps your ear in line with your shoulder when side lying. Memory-foam models with a subtle jaw cutout can reduce cheek pressure.
- Try a low-Fowler angle. Slip a wedge under your upper torso so your head and shoulders rise about 30 degrees. Clinical data from Zhong et al. showed fewer bruxism bursts in this position.
- Schedule jaw exercises. In a randomized trial by Karabicak Gul et al., simple open-close and side-glide drills lowered pain scores in as little as four weeks.
- Cut the late-night latte. Caffeine is a jaw-muscle stimulant. The ADA recommends a caffeine curfew of six hours before bed for grinders. Explore more on how caffeine affects bruxism.
- Warm up before lights out. A warm, moist towel on each cheek relaxes the masseter, making clenching less likely once you drift off.
- Keep airways clear. Nasal strips or a humidifier can reduce OSA-triggered clenching, as noted in the apnea review by van Looij et al.
Exercise matters too. Regular aerobic activity improves overall sleep quality, while postural workouts like yoga strengthen deep neck flexors that support the jaw. In the same trial, participants who combined jaw and posture routines reported better outcomes than those who focused on the jaw alone. Discover more about natural bruxism solutions like yoga and meditation.
If lifestyle hacks fail to quiet the pain after four to six weeks, move on to professional input. Think of home care as first aid, not a forever solution.
When to Seek Professional Help
Recurring morning jaw pain can morph from nuisance to constant ache. The Mayo Clinic recommends seeking evaluation when you notice any of these red flags:
- Pain lasts beyond two weeks despite self-care.
- Your jaw locks or you cannot open wider than two finger widths.
- Headaches or ear pain accompany the jaw soreness every day.
- You suspect sleep apnea (snoring, gasping, daytime fatigue).
Dental professionals may suggest an occlusal splint first. These custom acrylic guards cushion teeth and hold the jaw in a neutral spot. In the mandibular advancement device (MAD) realm, Ettlin and Mishra reviewed MADs for OSA and noted that while they reduce apnea events, they may introduce temporary TMJ discomfort. Close follow-up is essential to tweak fit and avoid trading breathing gains for jaw pain.
Other interventions include:
- Botulinum toxin: Limits muscle overactivity. A pilot trial by Taalat Gavrilă et al. confirmed modest pain relief, though cost and repeat injections are downsides.
- Physical therapy: Combines manual muscle release, ultrasound, and posture training.
- Cognitive behavioral therapy: Addresses stress triggers and sleep hygiene, often unnoticed drivers of nighttime clenching.
- Surgical consultation: Reserved for structural issues like disc displacement or degenerative joint disease unresponsive to conservative care.
Your provider may also order a sleep study to rule out OSA, especially if lifestyle changes fall flat. Treating the breathing disorder often reduces nocturnal jaw activity as a pleasant side effect.
Conclusion
Jaw pain that greets you with the alarm clock is rarely random. Research shows that how you position your head, neck, and jaw for seven or eight hours writes the morning pain script. Side-sleeping on a lofty pillow can shove the TMJ out of alignment, back sleeping without support may trigger airway-linked clenching, and stomach sleeping twists the whole setup. Mix in bruxism or a touch of sleep apnea and the plot thickens.
The upside is that position is fixable. A pillow swap, a gentle incline, and targeted jaw exercises offer meaningful relief for many people. Add professional tools like splints or physical therapy when needed, and most cases calm down without resorting to invasive measures.
Stay aware of your symptoms, experiment with supportive sleep gear, and consult a dentist or sleep specialist if pain persists. Your jaw does a lot of heavy lifting during the day. Give it a break at night so you can wake up ready to eat, talk, and grin without that nagging ache.