Exploring Hypnotherapy for Bruxism: Fact or Fiction?
Discover if hypnotherapy is a valid treatment for bruxism with scientific insights.
You heard the night-time scraping, or maybe your dentist spotted flattened enamel. Now you are deep-diving the internet wondering whether a session with a swinging pocket watch can stop your jaw from grinding. Before you book a hypnotherapy appointment, let’s look at the science, the hype, and everything in between.
This article pulls together peer-reviewed research, expert guidelines, and plain-language explanations so you can weigh the evidence for yourself. No crystals, no mysticism. Just data, humor, and practical takeaways.
Understanding Bruxism: Causes and Consequences
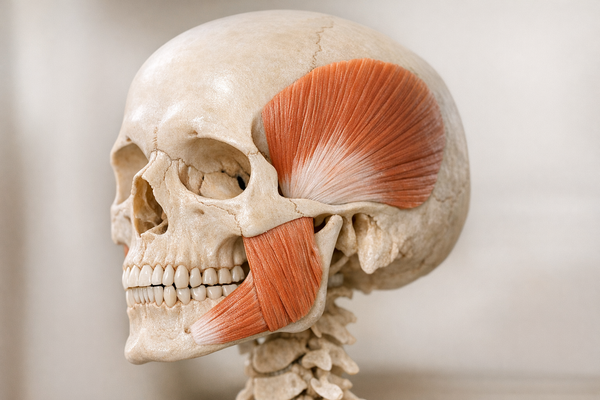
Bruxism is the medical term for the repetitive clenching or grinding of teeth. It can happen while you are awake (awake bruxism) or while you sleep (sleep bruxism). Either way, it can turn tooth enamel into chalk dust and leave your jaw muscles feeling like they ran a marathon.
How common is it? A sweeping bibliometric review mapped more than 4,000 publications and estimated that 8–31 percent of adults grind their teeth at night, depending on diagnostic criteria, as reported in a 2025 analysis by Doğan.
If you are an athlete, the odds tick even higher. A 2025 systematic review pooled data from 14 sports studies and found a bruxism prevalence of roughly 34 percent among competitive athletes, according to research led by de Sales et al. The theory is that high physical and mental stress during training spills over into night-time muscle activity.
Why does bruxism happen in the first place? Researchers point to a mix of factors:
- Central nervous system arousals during certain sleep stages (micro-awakenings in REM and non-REM stage 2 seem especially pivotal)
- Psychological stress and anxiety
- Caffeine, alcohol, and certain medications (for example, SSRIs) that tweak neurotransmitters
- Malocclusion (although evidence here is weaker than once believed)
- Obstructive sleep apnea, which often coexists with bruxism
Many people discover the habit only after “red-flag” clues: morning jaw stiffness, unexplained cracked fillings, or a bed partner’s complaint about midnight crunching. If pain radiates to the ear, or if you notice limited mouth opening (“lock-jaw”), fast-track a dental or orofacial pain consult.
The consequences extend beyond noisy nights:
- Tooth wear, fractures, and sensitivity
- Temporomandibular joint (TMJ) pain or clicking
- Headaches, especially in the temples
- Interrupted sleep for you and anyone within earshot
Left unchecked, chronic grinding can even loosen implants and crowns. Finite element analysis has linked bruxism-like forces to higher shear stress on dental hardware, as studied by Karip & Gök in 2026. So intervention is more than cosmetic vanity—your bite depends on it.
Traditional and Alternative Treatments for Bruxism
Your dentist’s first instinct may be to fit you with a mouthguard, but that is only one tool in the kit. Let’s line up the usual suspects—traditional and alternative—so you can see where hypnotherapy might slot in.
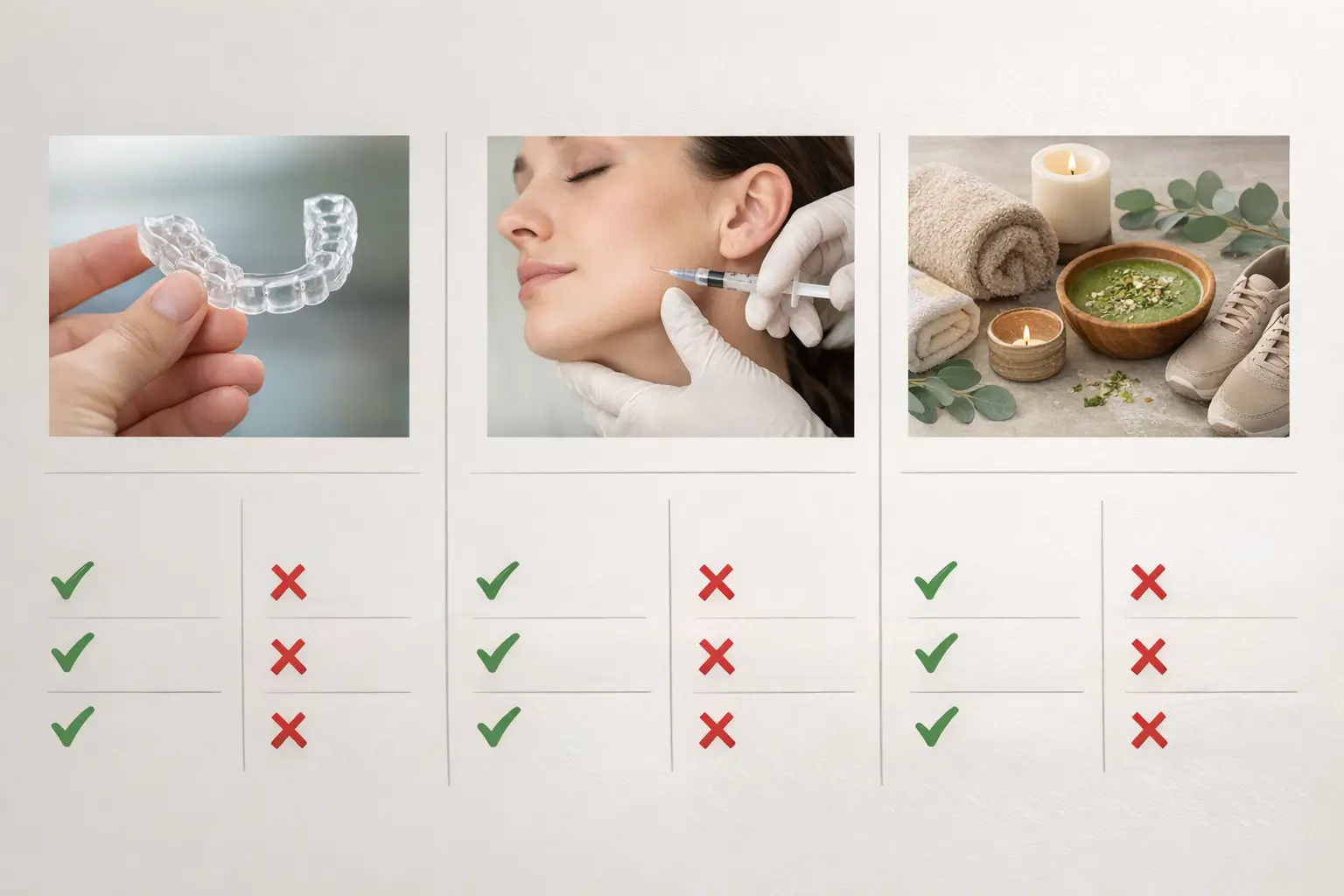
Occlusal Splints
Occlusal splints (also called night guards) are custom plastic appliances that sit between your upper and lower teeth. They do not stop the muscle contractions; instead, they spread the load and protect enamel.
How well do they work? A 2025 randomized clinical trial pitted splints against sleep hygiene coaching plus progressive muscle relaxation. After 12 weeks, both groups showed reduced subjective stress and grinding episodes, but there was no clear winner, according to Tandon et al. The takeaway: a splint helps physically, but stress management matters too.
Real-world tip: compliance can be the Achilles’ heel. Many users toss the guard aside after the third night because it feels bulky or dries the mouth. Ask your dentist about thinner hard–soft hybrids or lab-adjusted distal ramps that improve comfort. Over-the-counter “boil-and-bite” guards are cheaper but often too thick; ill-fit can actually worsen muscle tension.
Pros:
- Non-invasive, reversible
- Protects dental work
Cons:
- Does not treat root causes
- Can be expensive if custom made
- Needs regular cleaning and periodic replacement
Botulinum Toxin Injections
Botox for bruxism might sound like celebrity dental spa fluff, yet the evidence base is growing. Botulinum toxin type A weakens the masseter and temporalis muscles, lowering bite force.
A 2025 systematic review pooled 21 studies and concluded that botulinum toxin significantly reduced pain scores and muscle activity, although study designs were mixed and follow-up periods were short, as noted by Yacoub et al. A separate comprehensive review echoed those findings but flagged cost and occasional side effects like smile asymmetry, according to Węgrzecka et al.
Pros:
- Directly weakens overactive muscles
- Relief within days, lasting 3–6 months
Cons:
- Needs repeat injections
- Possible bruising or muscle weakness for chewing
- Costly out-of-pocket if insurance does not cover
Other Alternatives
Beyond plastics and needles, clinicians often recommend the following:
- Sleep hygiene tweaks: consistent bedtime, dim lights, no doom-scrolling in bed
- Progressive muscle relaxation: tensing and releasing muscle groups to lower baseline tension
- Cognitive-behavioral therapy (CBT): targets stress and anxiety triggers
- Biofeedback wearables: mini EMG stickers or headbands that buzz gently when jaw muscles activate, nudging you to unclench during the day
- Mandibular advancement devices: for those with sleep apnea (borrowed from apnea care guidelines such as the CHOICE trial)
Evidence for lifestyle measures is mixed because stress and sleep quality are hard to quantify, yet they carry virtually no side effects and improve overall health. Systematic reviews of bruxism management underline the importance of blending mechanical protection with behavioral change, as highlighted by Assiri et al. and Morales-Lastre et al.
The Science Behind Hypnotherapy
Now to the mind-bending part. Hypnotherapy combines focused attention, guided relaxation, and suggestion to modify behaviors or perceptions. You remain awake and in control. The goal is to access a mental state where positive suggestions sink in more easily.

How Hypnotherapy Works
Functional MRI studies show that hypnosis changes activity in brain regions linked to attention, body awareness, and pain perception. Think of it as temporarily turning down the mental noise so you can rewire habits without distractions.
Sessions usually run 45–60 minutes. The therapist guides you through progressive relaxation, narrows your focus, then delivers targeted suggestions—like, “Your jaw muscles feel loose and calm.” You may also learn self-hypnosis scripts to practice at home, reinforcing the new pattern.
Hypnotherapy in Medical Treatments
Clinicians already deploy hypnosis for chronic pain, irritable bowel syndrome, smoking cessation, and procedural anxiety. The National Center for Complementary and Integrative Health notes moderate evidence that hypnosis can reduce short-term pain and help some people quit tobacco. The American Psychological Association lists hypnosis as a tool in evidence-based behavioral medicine, especially when combined with CBT.
For dental scenarios, hypnotherapy has trimmed needle phobia and gag reflex. So the concept of applying it to bruxism is not a moon-shot, but does the data back it up? Let’s dig deeper.
Hypnotherapy for Bruxism: Current Research and Opinions
Search “hypnotherapy bruxism” in PubMed and you will find a handful of small studies, many dating back to the 1980s and 1990s. Sample sizes hover around 10–30 participants, often without control groups. Their general story: several weeks of hypnotherapy reduced reported grinding, sometimes verified by decreased wear on oral splints.
One illustrative case series from a university clinic followed eight patients who combined self-hypnosis audio tracks with nightly EMG logging. After four weeks, EMG bursts dropped by an average of 48 percent, and three participants discontinued their splints entirely. Yet the study lacked a sham-audio control, leaving room for placebo confounders.
Why so few trials? Funding priorities tend to favor pharmacologic or device-based solutions. Also, hypnosis research struggles with placebo controls—how do you sham-hypnotize someone convincingly?
Expert opinions vary:
- Proponents note that bruxism is tied to stress and arousal, domains where hypnosis shines. They reference case reports of patients who dropped from 80 grinding events per night to single digits after six sessions.
- Skeptics counter that most evidence is anecdotal, relies on self-reports, and lacks long-term follow-up. They worry about regression to the mean—symptoms sometimes ease naturally, and small trials can overstate benefits.
What do authoritative bodies say? The American Dental Association lists hypnosis under “emerging or complementary therapies,” noting insufficient high-quality evidence. The UK NHS echoes that stance but adds that hypnosis is considered safe when practiced by trained professionals.
Patient stories paint a mixed picture. Online forums brim with posts from users who swear by hypnosis tracks on their phones, while others saw zero change. Placebo effect? Possibly. But if the placebo comes with lower stress and better sleep, some patients are content.
The bottom line: we have encouraging but limited data, not yet strong enough for formal guidelines. More rigorously designed randomized controlled trials (RCTs) are needed—ideally with objective measurements like electromyography (EMG) sensors or bite force recorders.
Comparing Hypnotherapy with Other Bruxism Treatments
When you line hypnotherapy up against splints, Botox, and lifestyle tweaks, several themes pop out.
Efficacy. Systematic reviews of bruxism treatments highlight occlusal splints and botulinum toxin as the most evidence-backed options today, as noted by Assiri et al. Hypnotherapy sits lower on the evidence ladder, similar to meditation or biofeedback—promising, but under-studied.
Side effects. Hypnotherapy’s risk profile is mild. The main drawback is lost time or money if it does not work for you. Contrast that with Botox bruising, or the dental adjustments needed if a splint irritates gums.
Cost. A custom night guard can run $300–$800, plus adjustments. Botox averages $400–$600 per session, two to three times a year. Hypnotherapy prices vary—from $100 to $250 per session—and many therapists recommend 4–8 sessions. Over a year, the price gap narrows.
Root-cause angle. Hypnotherapy aims to retrain muscle memory and reduce stress arousal loops. Splints treat symptoms, not cause. Botox weakens muscles but does not address stress. So, in theory, hypnosis tackles upstream triggers. Whether that theory translates into durable outcomes remains to be proven.
Overall, a 2025 clinical management review urges dentists to adopt a multimodal approach: mechanical protection, behavioral intervention, and periodic reassessment, as highlighted by Morales-Lastre et al. Hypnotherapy could slot into the behavioral lane for patients motivated to give it a shot.
What the Future Holds for Hypnotherapy and Bruxism
Bruxism research is booming. An altmetric analysis shows rising public interest, with social media chatter spiking around new treatment studies, as noted by Rocha et al. That visibility may attract grants for larger hypnosis trials.
Wearable tech is another catalyst. Imagine pairing real-time EMG data from a smart mouthguard with app-based self-hypnosis prompts. Personalized feedback loops could measure improvement objectively, finally giving hypnosis the data points it needs.
Artificial intelligence might help too, tailoring hypnotic scripts to a user’s stress patterns, much like meditation apps now adapt to heart-rate swings. The future of hypnotherapy will likely be digital, data-driven, and integrated with behavioral coaching platforms.
Conclusion
So, is hypnotherapy for bruxism fact or fiction? Right now, it lives in a grey zone. The technique is plausible, low-risk, and backed by small but favorable studies, yet it lacks the robust evidence base that mouthguards and botulinum toxin enjoy.
If you are tired of grinding through nights (and dental bills), here is a practical roadmap:
- Start with a dental exam and, if possible, a sleep study to rule out apnea.
- Protect your teeth with a well-fitted splint while exploring stress-reduction methods.
- If traditional steps fall short, consider a certified hypnotherapist. Check credentials—look for training recognized by bodies like the British Society of Clinical Hypnosis or equivalent.
- Track progress objectively—daily jaw tension logs, follow-up dentist checks, or EMG devices if available.
- Reassess every six months. Combine approaches rather than staking everything on one method.
You deserve uninterrupted sleep and intact enamel. Whether that answer lies in plastic, protein toxin, or the power of suggestion is ultimately your call, armed with the evidence above.